CASE20230825_035
A Callenging Case in Acute Myocardial Infarction: Graft or Native Vessel
By Chih Hung Lai
Presenter
Chin Hung Lai
Authors
Chih Hung Lai1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
CASE20230825_035
ACS/AMI - ACS/AMI
A Callenging Case in Acute Myocardial Infarction: Graft or Native Vessel
Chih Hung Lai1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
61 year-old male has past history of hypertension, type 2 DM, atrial fibrillation and coronary artery disease after bypass surgery on 2005 (graft vein to left anterior decending artery, other graft vein to obtuse marginal branch of circumflex artery and sequentially to posterior descending artery of right coronary artery). The MDCT on 2013 showed patent of two graft vens. He was admiteed to our hosptial due to acue chest tightness and cold sweating.


Relevant Test Results Prior to Catheterization
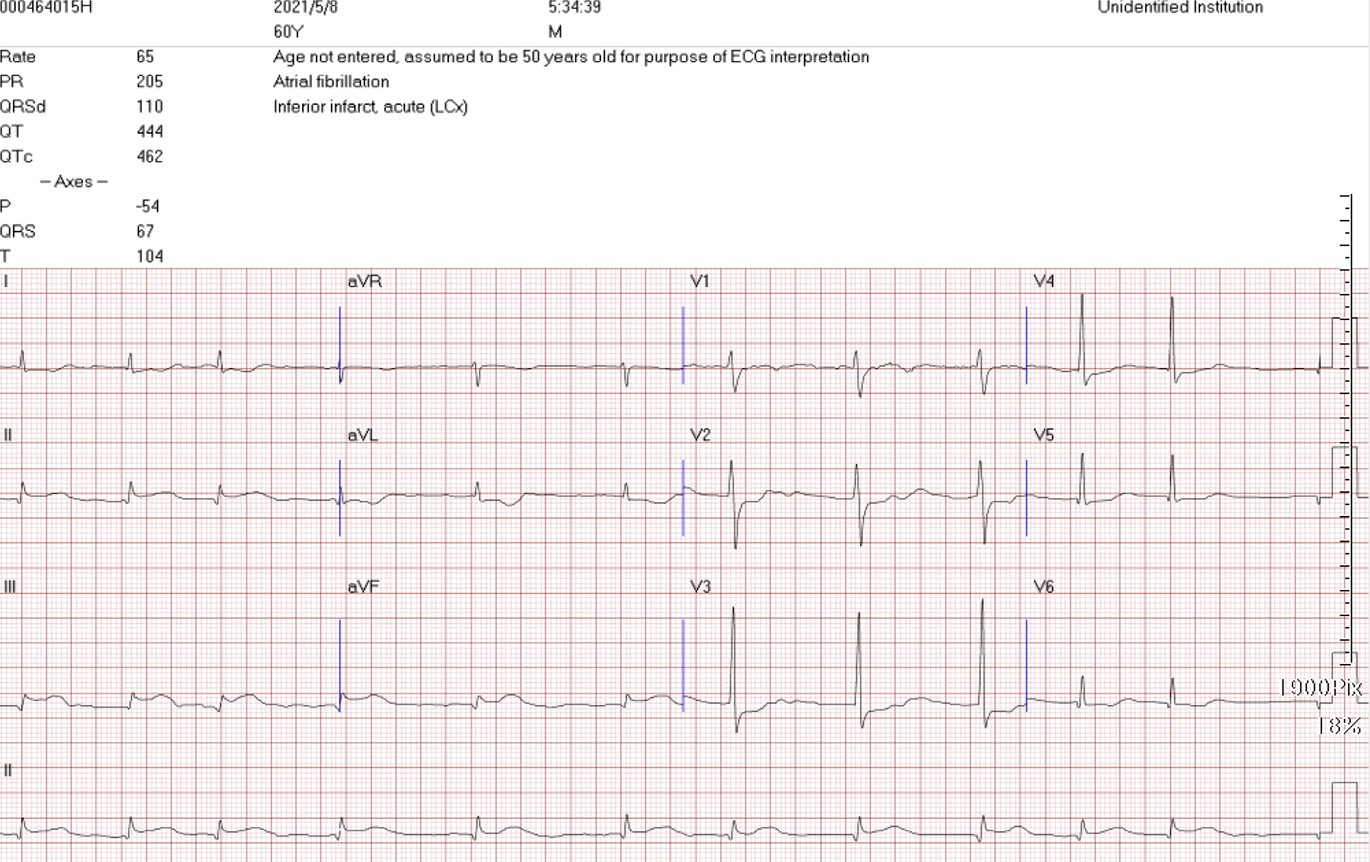
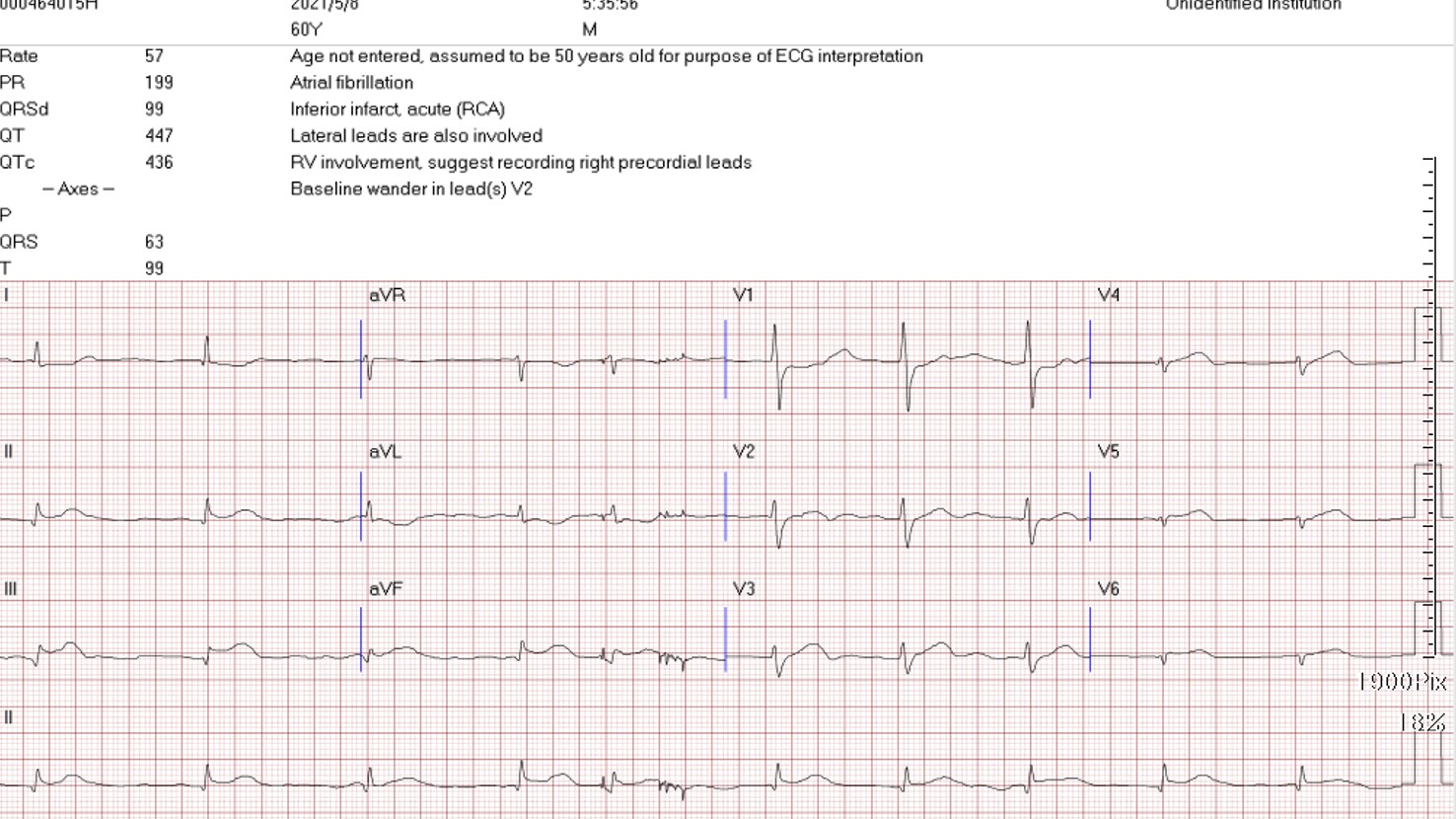
He had sudden chest pain and cold sweating in ealry morning, then, was admitted to our hospital and electrocardiogram showed inferior leads ST elevation and inferior wall STEMI was diagnosed. The primary PCI was initiated right away.
Relevant Catheterization Findings
The coronary angiography showed RCA-M chronic total occlusion (as prevoius MDCT) and graft vein to LAD was patent, as well the other graft vein to LCX-OM was patent, however, the sequential graft vein to PDA was total occlusion. The distal graft vein total occlusion is the culprit lesion of this inferior wall STEMI.
 2_RCA LAO.AVI
2_RCA LAO.AVI
GSV1 to LAD.AVI
GSV to OM to PDA.AVI
Interventional Management
Procedural Step
SAL 1/6 guiding cathter was engaged to graft vein ostium and a Fielder FC guide wire was advanced through graft vein to distal RCA. Then, maunal thrombus aspiration, distal IC injection Aggrastat (Tirofiban Hydrochloride), balloon dilation were used to remove huge thrmbus burden over distal graft vein. However, despite aggrassive procedures, huge thrombus persisted and the restored flow was intermittent, lesser than TIMI II flow (Video 3). Consideration of the possible graft failure (mora than 15 years) and poor dsital flow, we decided to recanalization of native right coronary artery. We used graft wire as distal guidance to do antegrad approach . By kissing wire technique, antegrade Gaia 3 GW was advanced cross RCA-M CTO into distal true lumen. However, APT microcathter could not cross CTO critical site. We used small balloon Trek 1.0mm to do dilation. However, the antegrade wire was pulled out while withdrawing the small balloon. After that, we could not antegrade wiring cross CTO again and into false lumen. Then, the regrade wire could cross CTO into antegrade APT microcathrer (Tip-in technique). The antegrade Finecross microcathter was advacend through retrograde GW into distal RCA-D true lumen successfully (Video 9). Then, antegrade system was changed to antegrade Sion blue GW and the RCA CTO site was seuquential dilation and stenting successfully (Video 10). The final RCA flow was restored.
3_poor flow to RCA.AVI
9_antegrade MC through retrowire into RCA-D.AVI
10_final RCA.AVI
Case Summary
Acute occlusion of GSVs is commonly associated with extensive
atherosclerotic and thrombotic burden, which increases the risk of distal embolization and no-reflow and, thus, death and myocardial infarction.Preferential intervention of the native coronary arterial circulation (rather than the occluded GSV) should be considered as an alternative route to reperfusing the myocardium and, if possible, will result in higher acute success and late patency rates. The main factors associated with PCI target vessel selection included: 1) the severity of SVG disease (which progressively worsens with longer interval from CABG); 2) the severity of native coronary artery disease.