CASE20230825_020
Never Underestimate the Side Branch :The Hybrid Strategy for Coronary Bifurcation Lesions
By Firman Dullah, Amir Aziz Alkatiri, Doni Firman, Arwin Saleh Mangkuanom, Nanda Iryuza
Presenter
Firman Dullah
Authors
Firman Dullah1, Amir Aziz Alkatiri2, Doni Firman2, Arwin Saleh Mangkuanom2, Nanda Iryuza2
Affiliation
National Heart Center Harapan Kita Jakarta Indonesia, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2,
View Study Report
CASE20230825_020
Complex PCI - Bifurcation
Never Underestimate the Side Branch :The Hybrid Strategy for Coronary Bifurcation Lesions
Firman Dullah1, Amir Aziz Alkatiri2, Doni Firman2, Arwin Saleh Mangkuanom2, Nanda Iryuza2
National Heart Center Harapan Kita Jakarta Indonesia, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2,
Clinical Information
Relevant Clinical History and Physical Exam
PatientInitials or Identified Number

Relevant Test Results Prior to Catheterization
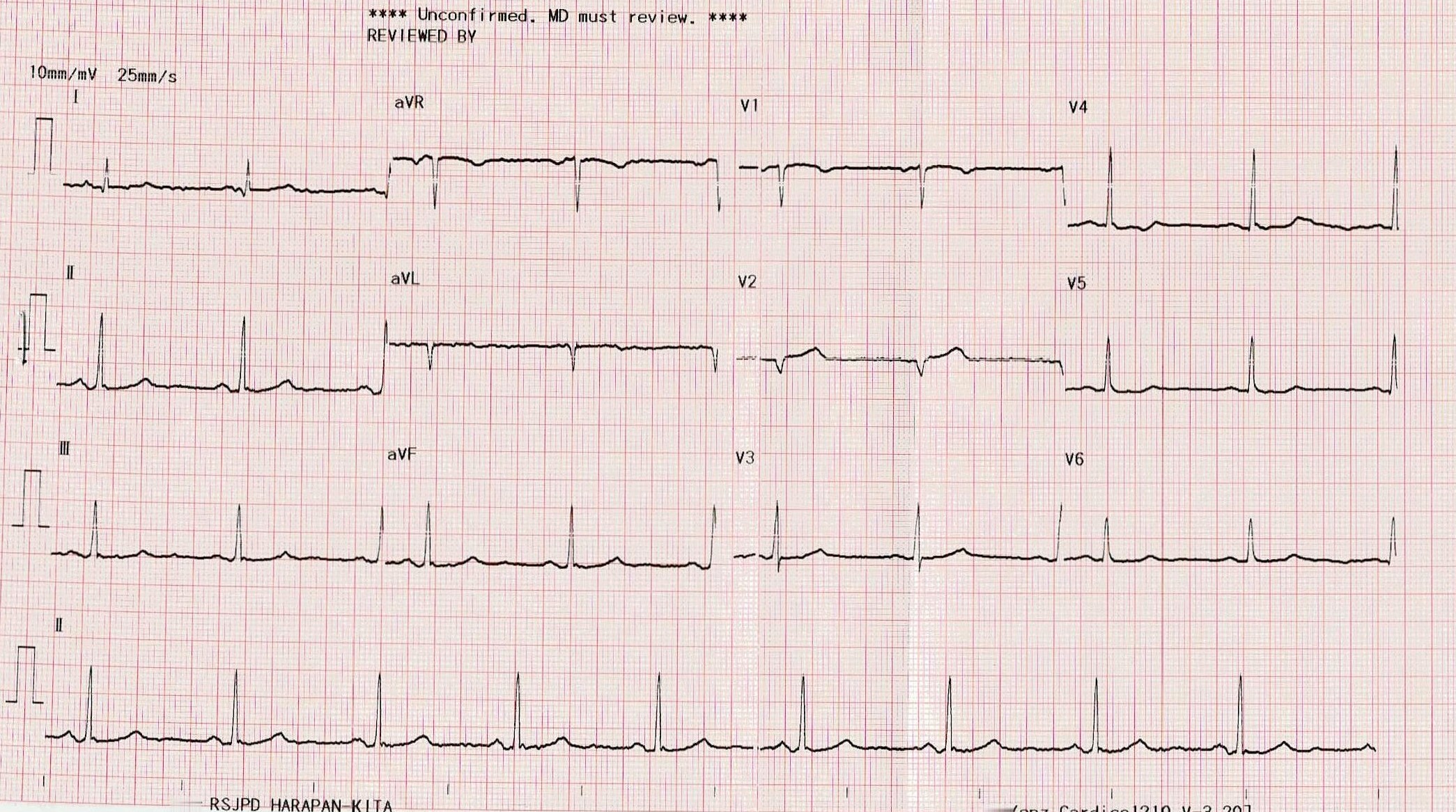
- ECG: Normal Sinus Rhythm withinnormal limit.
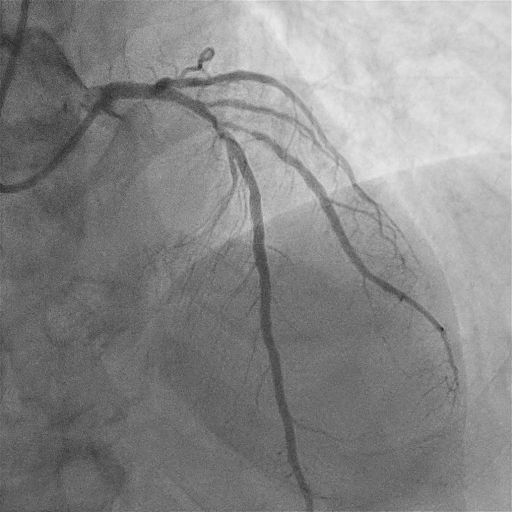
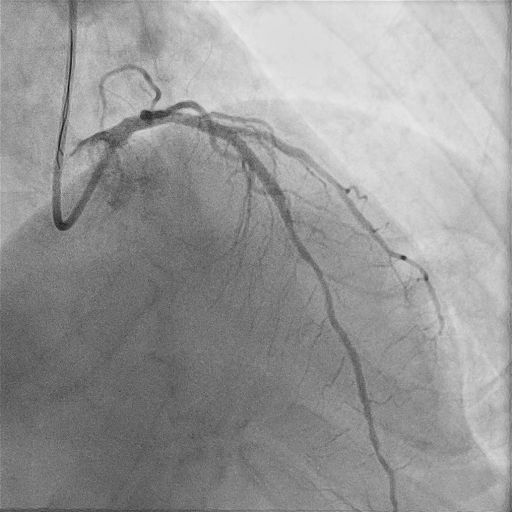
Relevant Catheterization Findings
AngiographyResult

Interventional Management
Procedural Step
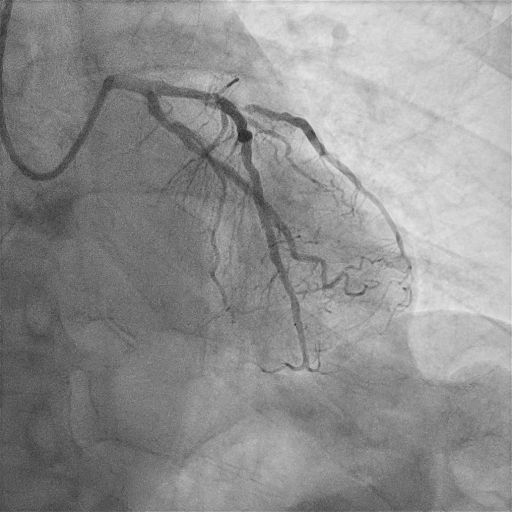
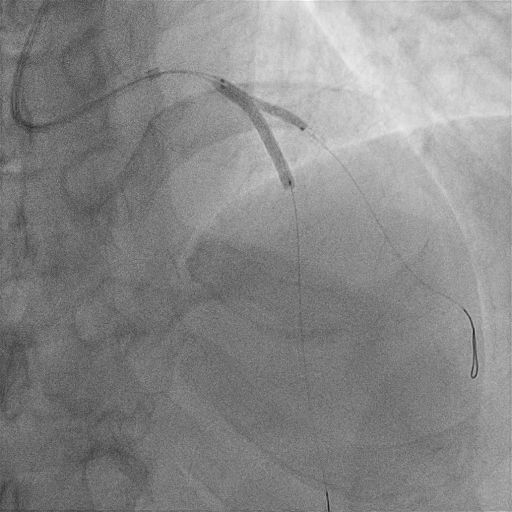
Firstly guided LCA with XB 3.5/6F. Then continued double wiring with Workhorse wire to distal LADand distal Side Branch (SB). Predilatationwith NC balloon 2.5 x 15 mm from mid to proximal LAD and continued to proximal SB. Implanted DES 3.0 x 28 mm but could not pass the proximalLAD. Rewiring with a new Workhorse wire to SB and perfomed buddy wire tothe distal LAD but stent still could not pass the LAD and continued predilatation again with NC balloon 2.5 x 15 mm.Implanted DES 3.0 x 28 mm and post dilatation with stent balloon at the proximal LAD. Buddy wire was removed and then exchange wire to SBand to LAD, followed Opening Struts with Semi-compliant balloon 2.0 x 15 mm atproximal SB then perfomed kissing balloon with NC balloon 2.5 x 15 mm atproximal SB and stent balloon 3.0 x 28 mm at proximal LAD instent. POT wasperformed in the proximal instent LAD with NC 3.25 x 12 mm. Followed rewiring the SB and LAD thenDCB implantation2.75 x 20 mm inflated for 1 minute at proximal SB.Perfomed with final kissing balloon with DCB balloon 2.75 x 20 mm in proximal SBand stent balloon 3.0 x 28 mm balloon in proximal LAD instent. Final POTwas performed with NC balloon 3.25 x 12 mm to proximal LAD instent but couldnot pass proximal LAD, so did the buddy wire again to distal LAD then continued with final POTwith NC balloon 3.25 x 12 mm. The final angiography results were good with TIMI 3 flow,no dissection and no residual stenosis.

Case Summary
Provisional Side Branch stentingstrategy is the default approach for the majority of bifurcation lesions, butoutcomes of SB is suboptimal.The Drug Coated Balloon (DCB) improving SB outcomesattracts an increasing attention, the hybrid strategy facilitates treatment ofDCB andstent for bifurcation lesions. This case demonstrated the hybrid strategy in bifurcation lesion with DCB.