CASE20230824_002
Image Guided LAD ISR CTO PCI
By Sanjeev Gera
Presenter
Sanjeev Gera
Authors
Sanjeev Gera1
Affiliation
DNB Cardiology, India1,
View Study Report
CASE20230824_002
Complex PCI - CTO
Image Guided LAD ISR CTO PCI
Sanjeev Gera1
DNB Cardiology, India1,
Clinical Information
Relevant Clinical History and Physical Exam
2 years old male, presented with hypertension & diabetes. Post PTCA LAD and Left Circumflex in 2018. Presented with refractory angina on exertion from 3 months. TMT positive and EjectionFraction 55%. Failed PTCA to LAD 2 months back.
Relevant Test Results Prior to Catheterization
CBC, KFT, Viral Marker, RBS, Pre ECG, Urine Iron, Chest X Ray, Echo, PTI NR, APTT
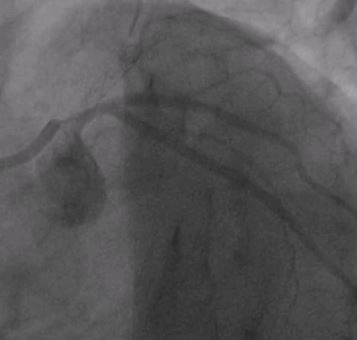
Relevant Catheterization Findings
Proximal ambiguous cap at LM Bifurcation. Long lesion, Distal Vessel normal with JCTO score 3. Collaterals getting filled by septal.
Interventional Management
Procedural Step
LMCA was hooked with XB 3.5 7F Guiding Catheter. Lesion tried to cross with fielder XT and Gaia II with support of Crusade Microcatheter, but could not be crossed due to ambiguous proximal cap. IVUS manual pullback done from Ramus to LM & transducer kept at ostium of ramus and LAD cab was observed at 5 O clock. Then another guide JL 3.5 7F hooked in LMCA as a Ping-Pong technique to poke the LAD lesion with Gaia III with support of micro catheter. After Gaia III, lesion got crossed and Gaia III wire exchange with workshorse wire. After crossing lesion sequentialpredialation was done and 2 DES were deployed.
 GAIA II.mp4
GAIA II.mp4
Case Summary
The case highlights the importance of imaging in ambigeous proximal cap in CTO intervention. IVUS guided navigation of proximal cap of LAD ISR CTO resulted in successful LAD PTCA. Other uses of IVUS in CTO IVUS guided wiring at proximal ambiguous cap / Stumpless CTOIVUS guided penetration from subintimal space.R Cart