CASE20230823_010
STEMI With a Midway Stone
By Choutchung Tinakorn Na Ayudhya, Suphot Srimahachota
Presenter
Choutchung Tinakorn Na Ayudhya
Authors
Choutchung Tinakorn Na Ayudhya1, Suphot Srimahachota1
Affiliation
King Chulalongkorn Memorial Hospital, Thailand1,
View Study Report
CASE20230823_010
ACS/AMI - ACS/AMI
STEMI With a Midway Stone
Choutchung Tinakorn Na Ayudhya1, Suphot Srimahachota1
King Chulalongkorn Memorial Hospital, Thailand1,
Clinical Information
Relevant Clinical History and Physical Exam
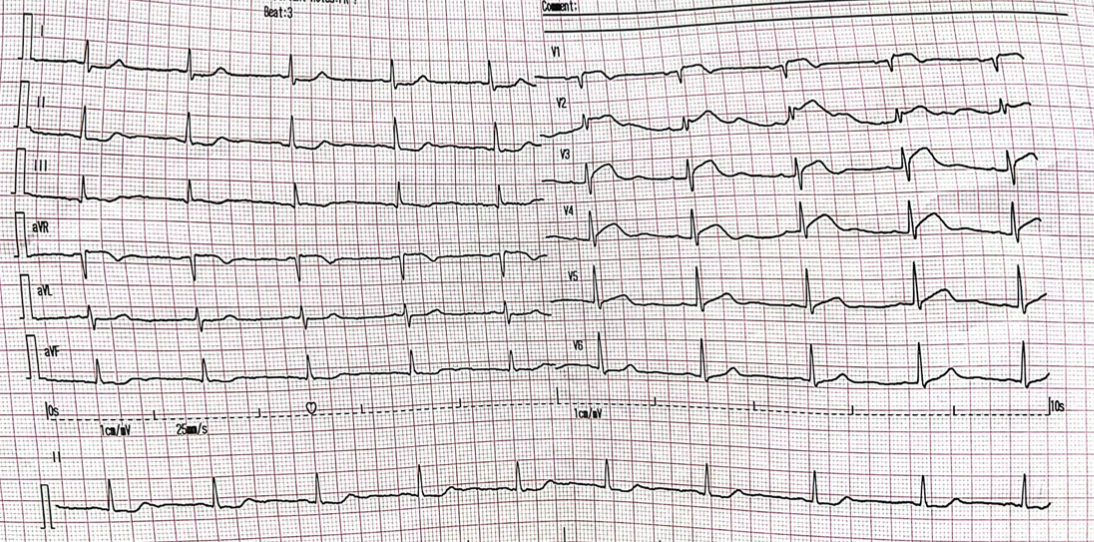
A 65 year old female without known underlying disease. She was an active smoker. She presented with acute typical angina at rest for 4 hours PTA without orthopnea or PND. At ER ECG 12 leads showed sinus rhythm rate 90/min with ST elevated in V1-V4. STEMI fast track was activated. Physical examination showed BP 112/90 mmHg, HR 90/min RR 16/min, RS no crepitation, CVS normal S1S2 no murmur. She received ASA gr V 1 tab and Ticagrelor (90) 2 tabs and Heparin 4500 units IV and was sent to cath lab
Relevant Test Results Prior to Catheterization
Echo bedside: LVEF 60% by Biplane with RWMAs. Hypokinesia to akinesia at mid to apical segment of anterior and septal wall without thinning of myocardium. Mild MR. No pericardial effusion.
 IMG_0765.MOV
IMG_0765.MOV
IMG_0764.MOV
IMG_0766.MOV
Relevant Catheterization Findings
CAG : Single vessel disease. 70% stenosis at proximal LAD. 100% thrombotic stenosis at mid LAD. There were collaterals from PL to LAD.
IMG_0767.MOV
IMG_0768.MOV
IMG_0769.MOV
Interventional Management
Procedural Step
PCI to mid LAD was done using 6Fr JL 3.5 guiding catheter. Run-through wire advanced into distal LAD. CAG showed TIMI 2 flow in distal LAD with some thrombi at mid LAD. 2 doses of weight based Eptifibatide were given IC. Pre-dilated was done with SC balloon 2.0x15 mm at mid LAD at 14 ATM. 2.5x30 mm DES was tried to advance to mid LAD but could not pass lesion at mid LAD. Buddy wire, Guide extension were tried but not success. Pre-dilatation was done with SC balloon 2.25x6 mm at proximal to mid LAD at 14 ATM but balloon still could not pass mid LAD lesion. Stent boost showed calcified nodule at mid LAD. Angiogram showed dissection at proximal LAD without limiting flow to LAD. Patient developed hypotension and chest pain IABP was inserted and guiding was changed to XB 3.0 IVUS was done which showed dissection and calcified nodule at mid LAD. Due to dissection, Rotablation was contraindicated. Buddy wire was done and NC balloon 2.5x15 mm could passed to mid LAD and inflated at 20 ATM. Pre-dilated was done with NC balloon 3.0x15 mm at 14 ATM to mid LAD. We still could not deliver stent across mid LAD so anchoring technique with guideextension catheter to distal LAD and we could deliver DES 2.5x30 mm at proximal to mid LAD and inflated at 18 ATM. Post dilated was done with NC balloon 3.0x15 mm.
IMG_0770.MOV
IMG_0771.MOV
IMG_0776.MOV
Case Summary
STEMI patient may had acute ontop of chronic lesion even though patient had no underlying disease. Multiple methods may be required to correct balloon/ stent uncrossable lesion such as increase guiding support, buddy wire and guide extension. Calcified lesion with contraindication for rotational atherectomy such as evidence of dissection, balloon based approach is still doable.