CASE20230821_006
"Beyond the First Episode: MINOCA's Unforeseen Path to Re-infarction and True Obstruction"
By Norhaliza Am Haris, Ahmad Farhan Abdul Hamid
Presenter
Norhaliza Am Haris
Authors
Norhaliza Am Haris1, Ahmad Farhan Abdul Hamid1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
CASE20230821_006
Adjuctive Procedures - Adjuctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
"Beyond the First Episode: MINOCA's Unforeseen Path to Re-infarction and True Obstruction"
Norhaliza Am Haris1, Ahmad Farhan Abdul Hamid1
National Heart Institute, Malaysia1,
Clinical Information
Relevant Clinical History and Physical Exam
MH, 32 years old man with no risk factors for CAD presented in November 2022 with ischemic chest pain for 2 days. He was treated for NSTEMI and underwent coronary angiogram that revealed unobstructed coronary arteries but ectatic RCA. His CMRI revealed previous myocardial infarction involving distal RCA with non-obstructive coronary artery disease (MINOCA). He was discharged well however presented again in June 2023 with acute inferior STEMI Killip 1. Physical examinations were unremarkable.
 pre1.avi
pre1.avi
pre2.avi
Relevant Test Results Prior to Catheterization
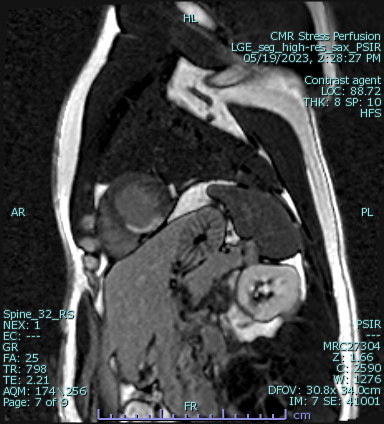
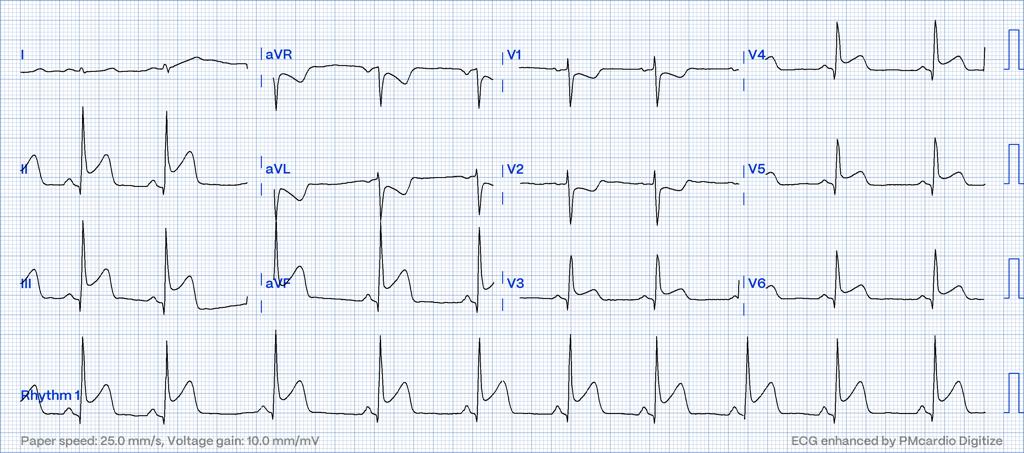
Previous ECG during NSTEMI showed T wave inversion at inferior leads. Raised troponin levels, LDL 3.3mmol/L, HbA1C 5%. Echocardiogram showed LVEF 54%, normal valves. Cardiac MRI in May 2023(6 months from index event) revealed findings of previous myocardial infarction involving distal RCA territory with non-obstructed coronary arteries (MINOCA). No evidence of stress induced ischemia and no microvascular dysfunction. He admitted again in June 2023 with ST elevation of the inferoposterior leads.
echo.avi
Relevant Catheterization Findings
Left Main stem: Normal.Left anterior descending artery: mild myocardial bridging at mid segment.Left circumflex artery: normalRight coronary artery: total occlusion at mid segment with TIMI 0 flow and huge thrombus burden
pre3.avi
pre4.avi
pre5.avi
Interventional Management
Procedural Step
JR 3.5 6Fr as guiding catheter. Lesion crossed with runthrough floppy wire. Multiple big red thrombi aspirated with thrombectomy by using EXPORT catheter, done at multiple times. Flow established but still TIMI 2 flow distally. Decided to give intracoronary aggrastat (tirofiban) for 3 minutes. Flow still poor, intracoronary adenosine 100mcg given. Flow became better subsequently. Patient however developed idioventricular rhythm and then sustained ventricular tachycardia, reverted to sinus rhythm after 3 times of defibrillation of 200J. Thrombus burdens still high, aspirated again with EXPORT catheter however thrombus propagated to distal PDA and not reachable for thrombectomy. Good TIMI 3 flow established eventually with no dissections. Mild disease at mid segment treated with medication. Stent was not put due to the heavy thrombus burden. Decided to stop the procedure and continue with IV aggrastat maintenance. Hemodynamically unsupported throughout the procedure.
post1.avi
post2.avi
post3.avi
Case Summary
Reinfarction following MINOCA carries high mortality and morbidity to the patient. Aggressive secondary preventive measures is therefore is very crucial after the first event which was likely due to spontaneous thrombolysis following plaque disruption or thrombus formation. Intracoronary imaging like IVUS or OCT helps to identify the mechanisms behind it so that specific therapies can be initiated to treat the underlying cause. Thrombectomy remains the mainstay of treatment of large coronary thrombus. Putting a stent in a ectatic coronary artery with large thrombus burden confers a high risk of reocclusion hence we decided to treat it with anticoagulation and potent antiplatelets.