CASE20230815_001
When Right Not Always Right: Primary PCI in Anomaly Ostium
By Rendra Mahardhika Mahardhika, Taofan Taofan, Doni Firman, Amir Aziz Alkatiri, Arwin Saleh Mangkuanom, Nanda Iryuza
Presenter
Rendra Mahardhika
Authors
Rendra Mahardhika Mahardhika1, Taofan Taofan2, Doni Firman3, Amir Aziz Alkatiri3, Arwin Saleh Mangkuanom3, Nanda Iryuza3
Affiliation
Airlangga University Indonesia, Indonesia1, National Cardiovascular Harapan Kita Hospital, Indonesia2, National Cardiovascular Center Harapan Kita, Indonesia3,
View Study Report
CASE20230815_001
ACS/AMI - ACS/AMI
When Right Not Always Right: Primary PCI in Anomaly Ostium
Rendra Mahardhika Mahardhika1, Taofan Taofan2, Doni Firman3, Amir Aziz Alkatiri3, Arwin Saleh Mangkuanom3, Nanda Iryuza3
Airlangga University Indonesia, Indonesia1, National Cardiovascular Harapan Kita Hospital, Indonesia2, National Cardiovascular Center Harapan Kita, Indonesia3,
Clinical Information
Relevant Clinical History and Physical Exam
Patient initials: Mr. R
A 55-year-old male, who was obese and a heavysmoker, presented to the Emergency Room (ER) with chest pain that had persistedfor five hours prior to admission. He was diagnosed with Inferior Acute STElevation Myocardial Infarction (ACS-STEMI). His vital signs upon arrival atthe ER were a blood pressure of 140/90 mmHg and a heart rate of 90 bpm. Therewere no rales, and his peripheral perfusions were normal
Relevant Test Results Prior to Catheterization
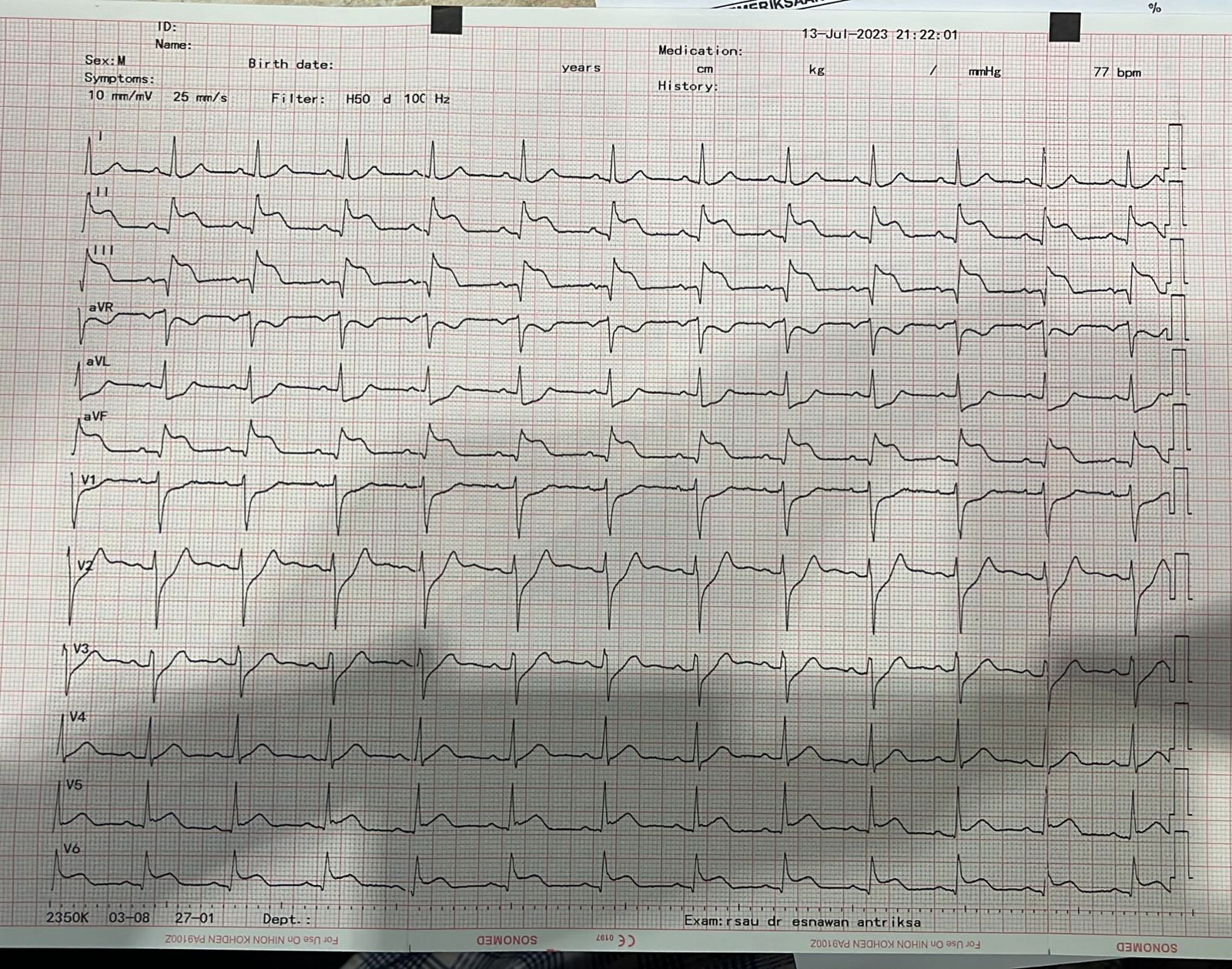
- ECG: Normal SinusRhythm, with ST Elevation in II-III-AVFEchocardiography: Left Ventricular EjectionFraction (LVEF) measured at 48%, with a regional wall motion abnormality at thebasal mid-inferior region. Right Ventricular (RV) function appeared normal (Tapse2.1 cm).Blood Count: Hemoglobin (Hb) level of 16.1 g/dL,White Blood Cell count (WBc) of 11000 /µL, Platelet count of 191.000 /µL, Urea level of 11.3 mg/dL, and Creatininelevel of 0.71 mg/dL
Relevant Catheterization Findings
Angiography Result
 LAO RCA.mp4
LAO RCA.mp4
Caudal.mp4
Cranial.mp4
Interventional Management
Procedural Step
1. Looking For RCA Ostium
RAO Caudal ostium.mp4
DES Implantation.mp4
Final Result.mp4
Case Summary
This case underscores the significance of encountering rare anomalies, such as the Ostium RCA anomaly, in routine daily practice. Thinking quickly about all possibilities, particularly within emergency settings, remains a pivotal skill for every Cardiac Interventionist. The pivotal role of three-dimensional(3D) perspective is highlighted, serving as a crucial guide when confrontinganomalies. It serves as a poignant reminder that the approach to PCI procedures can markedly differ when encountering such anomalies compared to standard PCI practices.