CASE20230712_003
A Challenging Case: Defer PCI Strategy Is Appropriate for Acute Infarction of Saphenous Vein
By Tuan Long Nguyen
Presenter
Tuan Long Nguyen
Authors
Tuan Long Nguyen1
Affiliation
Tam Anh Hospital, Vietnam1,
View Study Report
CASE20230712_003
ACS/AMI - ACS/AMI
A Challenging Case: Defer PCI Strategy Is Appropriate for Acute Infarction of Saphenous Vein
Tuan Long Nguyen1
Tam Anh Hospital, Vietnam1,
Clinical Information
Relevant Clinical History and Physical Exam
A male patient aged 56, with a history of mechanical mitral valve replacement and CABG surgery a decade ago, presented at the hospital with complaints of left-sided chest discomfort. His symptoms included left-sided chest pain, dyspnea, sweating, atrial fibrillation, a heart rate of 37 beats per minute, and blood pressure of 110/60mmHg.
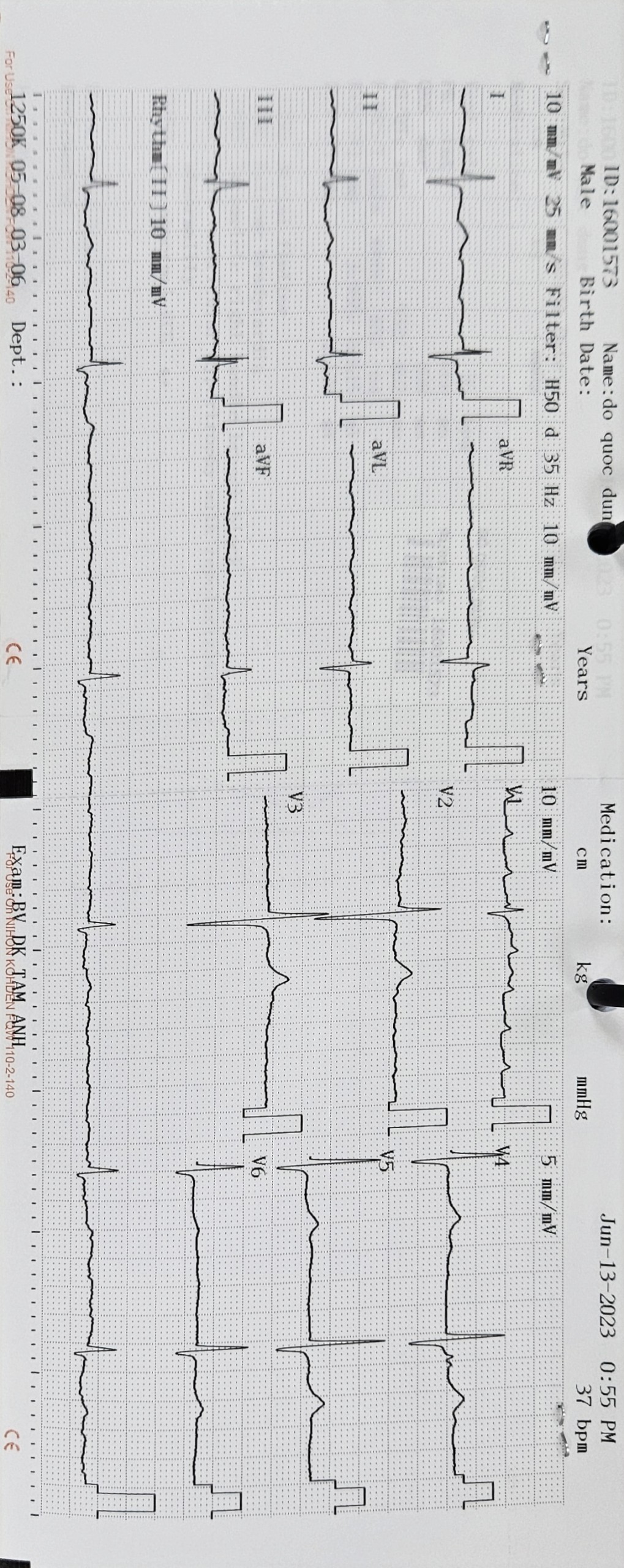
Relevant Test Results Prior to Catheterization
The ECG showed atrial fibrillation and a 3rd-degree AV block. The echocardiography revealed an EF of 63%, dyskinesia in the inferior wall, and normal mechanical heart valve function.The INR 3.16Creatinine: 78,4 umol/lUre: 7,2 mmol/lK+: 3,98 mmol/lTroponin Ths: 14,9 pg/mL
Relevant Catheterization Findings
The results of the coronary angiography:
 MOVIE-0002.mp4
MOVIE-0002.mp4
MOVIE-0013.mp4
MOVIE-0023.mp4
Interventional Management
Procedural Step
We successfully aspirated the thrombus of the SV bypass using right femoral artery access (JR4.0, Runthrough 0.14, and Export™ catheter). This allowed us to restore the flow of the SV to the PDA. The patient was subsequently transferred to the Department of Cardiology for Lovenox, aspirin, and clopidogrel treatment. A repeat coronary angiography was done after three days due to persistent chest pain. The angiography showed that the SV bypass was blocked again. CTO intervention of the RCA was attempted using the right radial access, AL 0.756F, Runthrough 0.14. However, guiding into the RCA ostial was challenging, so a floating technique was employed with the help of a Finecross micro-catheter and a highly flexed second curve (over 90 degrees). Fortunately, driving through the lesion (with Runthrough) was not difficult. However, passing the ball over the lesion was challenging. Incremental balloons expanded the lesion with 10-16 atm pressure, including Pantera Pro 1.25x15mm, Pantera Pro 1.50x10mm, and PanteraPro 2.0x15mm. After measurement, stenting was done from the PDA to the RCA ostial using Cruz 2.5 x 48mm, Onyx 2.75 x 38mm, and Cruz 3.5 x 20mm with pressure 8-10 atm. Post-dilation was performed using Raiden 2.75x15mm, Pantera Leo 3.0 x 15mm, and Raiden 3.5 x 20mm balloons with pressure 14 to 24 atm. The flow after the intervention was satisfactory with TIMI3.
MOVIE-0026.mp4
MOVIE-0009.mp4
MOVIE-0090.mp4
Case Summary
Deferring stenting forpatients with acute coronary syndrome caused by degenerated saphenous veinocclusion is not recommended due to the significant risk of re-occlusion.Trying to revascularize the native vascular system may be challenging, but itmay result in good outcomes for the patient.