CASE20230819_001
An Interesting Bifurcation Stenting Technique Case With Supporting Imaging
By Trung Minh Tran, Huynh Trung Cang
Presenter
Trung Tran
Authors
Trung Minh Tran1, Huynh Trung Cang1
Affiliation
Kien Giang General Hospital, Vietnam1,
View Study Report
CASE20230819_001
Complex PCI - Bifurcation
An Interesting Bifurcation Stenting Technique Case With Supporting Imaging
Trung Minh Tran1, Huynh Trung Cang1
Kien Giang General Hospital, Vietnam1,
Clinical Information
Relevant Clinical History and Physical Exam
medical history: hypertension, non-ST elevation myocardial infarction and triple coronary disease with one stent in RCA in 2022, 1 stent in LCx in January 2023, 70% narrowing in mid LAD and 90% in first diagonalphysical exam: patient had angina 3/10, no dyspnea, no rales, normal heart rate

Relevant Test Results Prior to Catheterization
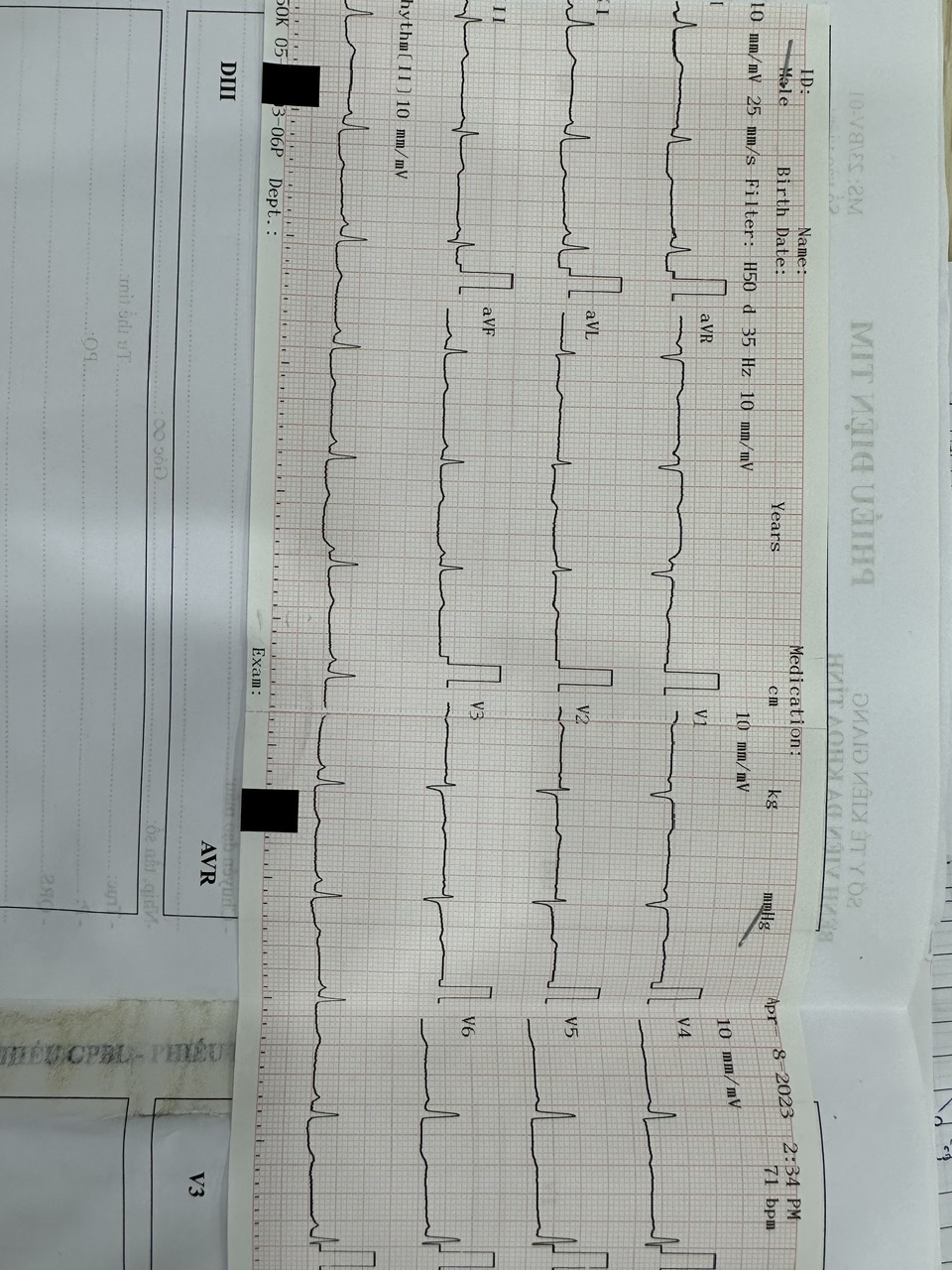
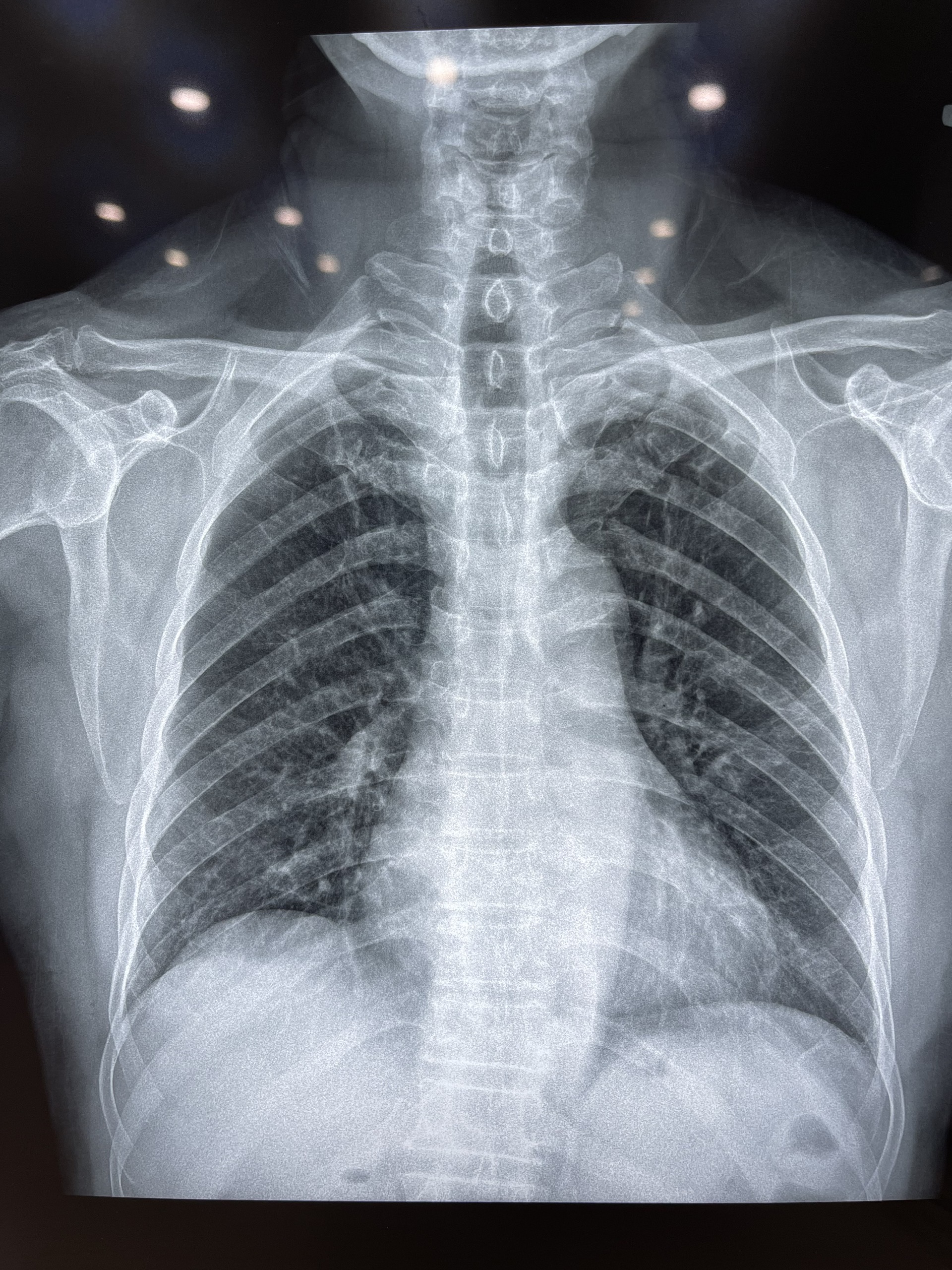
electrocardiogram showed sinus rhythm with normal heart rate, mild anterior ischemia echocardiogram demonstrated normal LVEF of 60 percent, no wall motion abnormalitieselectrolyte tests were normal and cardiac troponin was normalchest xray was normalabdominal echo was normal

Relevant Catheterization Findings
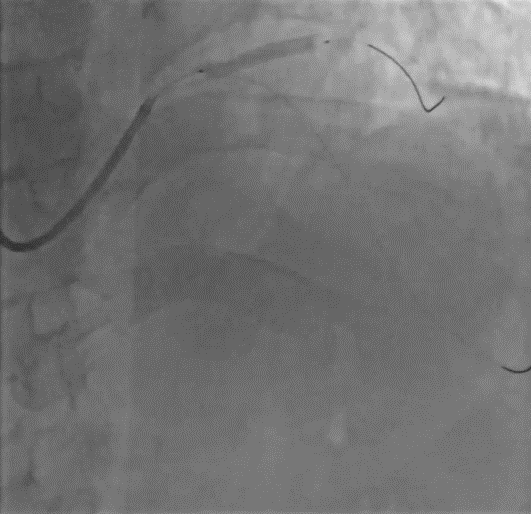
catheterization showed patent stent in left circumflex and right coronary artery, 70 percent narrowing in mid left anterior descending artery and 90% narrowing in first diagonal and that a bifurcation with medina 1,1,1


Interventional Management
Procedural Step
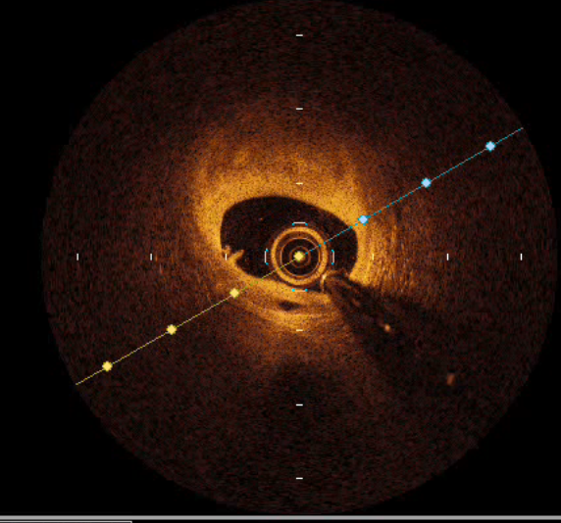
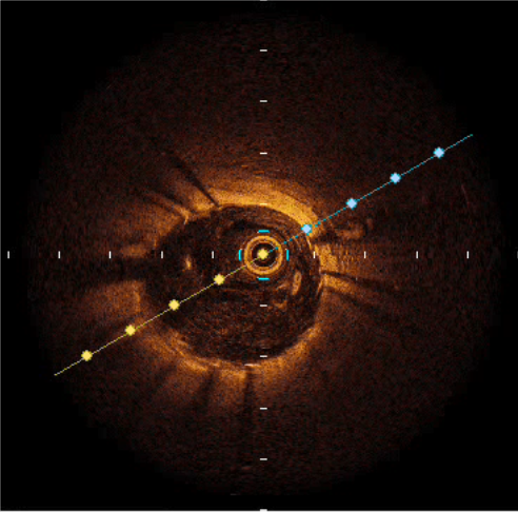
procedural steps in my casewe did distal radial artery access, EBU 6F guiding catheter, two Runthrough NS 0.014inch guidewires. After going 2 guide wires through distal left anterior descending and distal first diagonal , we did pre PCI optical coherence tomography to identify morphology, lesion length and diameter reference. And we got fibrous plaque and mild calcified plaque in 2 lesions, length from mid LAD to proximal LAD approximately 28mm, distal diameter was 3.3mm and proximal diameter was 4.33mm and length from first diagonal to mid LAD was 20mm and diagonal diameter was 2.93mm. So we decided to did a culotte technique bifurcation scenting. First we predicated first diagonal by 2.0x20mm compliant balloon at 12atm, we deployed 3.0x26mm DES stent in first diagonal - mid LAD at 16atm (3.20mm). After that we rewired Runthrough NS from proximal LAD to distal LAD. We predicated mid LAD by 2.0x20mm compliant balloon. Then we deployed 3.5x30mm DES stent from proximal LAD to mid LAD at 12atm (3.45mm). We used 2 NC ballon, 3.25x15mm in proximal LAD and 3.0x15mm in first diagonal and inflated 20bar simultaneously. And we did POT by 3.5x15mm NC balloon at 21atm. We did post PCI optical coherence tomography to assess the result of stenting. We had a good stent apposition and expansion, no dissection. We did final pictures for the procedure.


Case Summary
we had a difficult bifurcation lesion. So we decided to use optical coherence tomography to guide the procedure and we got the good result. And we thought that optical coherence tomography guided PCI will facilitate to balloon, stent selection and help the successful procure. We recommend to use optical coherence tomography in the bifurcation stenting to guide the PCI.