CASE20230816_002
Relentless Pursuit
By Kogulakrishnan Kaniappan, Kumara Gurupparan Ganesan
Presenter
Kogulakrishnan Kaniappan
Authors
Kogulakrishnan Kaniappan1, Kumara Gurupparan Ganesan1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
CASE20230816_002
Vascular Access and Closure - Vascular Access and Closure
Relentless Pursuit
Kogulakrishnan Kaniappan1, Kumara Gurupparan Ganesan1
National Heart Institute, Malaysia1,
Clinical Information
Relevant Clinical History and Physical Exam
68 years old Female
ECG in ED : Sinus rhythm, LAD, no ST elevation
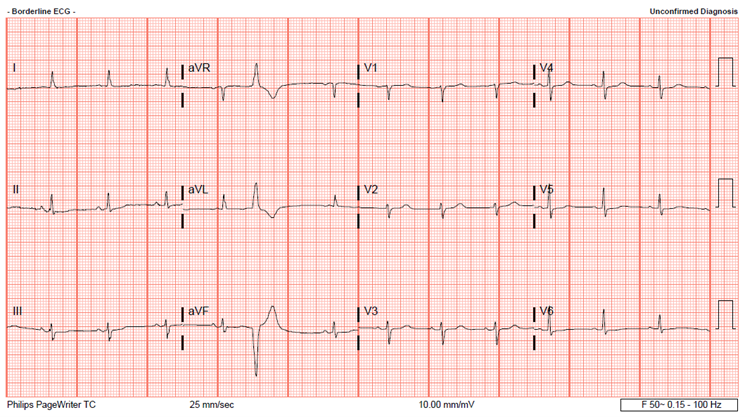
ECG in ED : Sinus rhythm, LAD, no ST elevation
Relevant Test Results Prior to Catheterization
Investigations : FBC : WCC 9.5 / Hb 11.4 / PLt 302
Echocardiography :
Relevant Catheterization Findings
Right femoral approach ; single puncture under fluoroscopy / USG guided
Interventional Management
Procedural Step
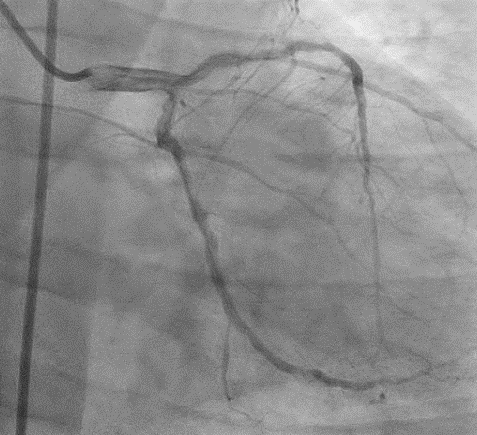
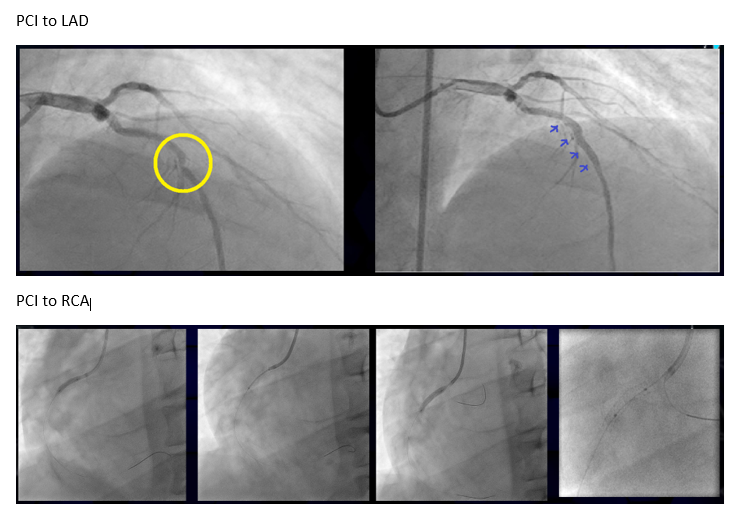
QFR LAD prePCI showed ischemia at 0.74.Decided forPCI to LAD.
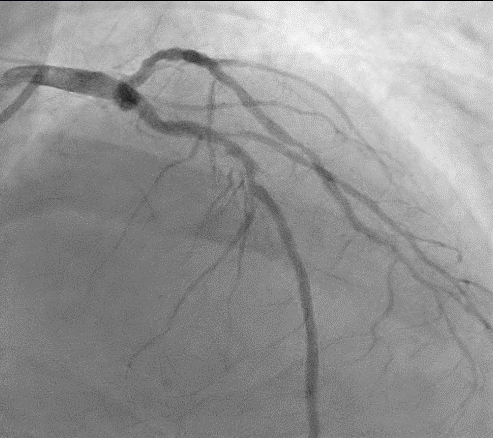
 rfa perforation.avi
rfa perforation.avi
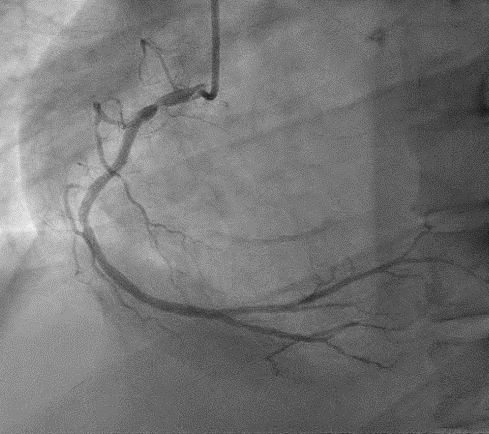
final results post covered stent.avi
Case Summary
This case highlights few salients points 1. Femoral access complication can occurs despite precaution taken with puncture done under flouroscopy and ultrasound guided2. Patient developed access complication despite initial femoral shot did not show any signs of extravasation3. It is critical for clinician to have high index of suspicion in high risk groups, especially in females, ESRF, calcified vessel, poor vessel wall compliance, advanced age, larger sheath, peripheral artery disease 4. The importance of emergency PTA and covered stent placement in time sensitive manner was crucial to save this patient's life