
CASE20210828_007
Glide through the Narrow Path
By ,
Presenter
Yee Sin Tey
Authors
1, 1
Affiliation
, Malaysia1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Glide through the Narrow Path
1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
L
Relevant Clinical History and Physical Exam
74 years old lady had underlying diabetes mellitus, hypertension and dyslipidaemia. She presented with recurrent admission for congestive heart failure and nstemi in last two months. Upon admission, she was hemodynamically stable. Clinical examination was unremarkable. Coronary angiogram was performed and subsequently she was referred to us for complex coronary angioplasty as patient was turned down by cardiothoracic surgeon for cabg.
Relevant Test Results Prior to Catheterization
Echocardiogram reviewed LVEF 15-20%. LVIDD 5.8cm. Global hypokinesia with moderate secondary mitral regurgitation.Technetium scan showed non viable at apical area.
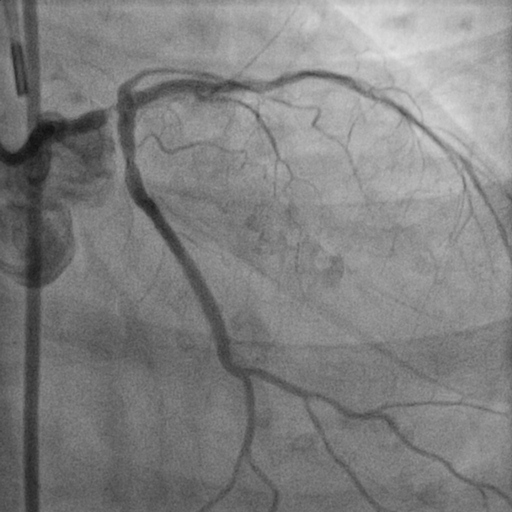
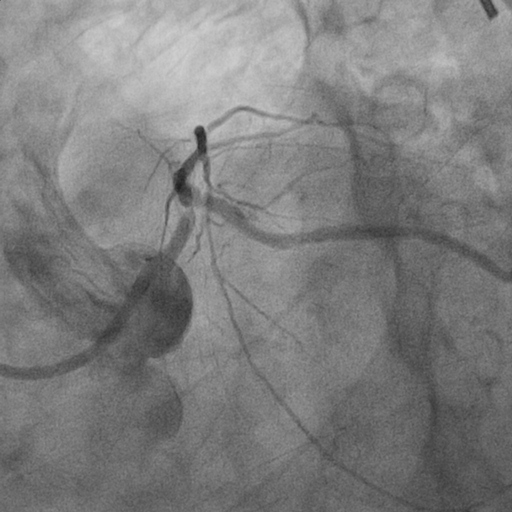
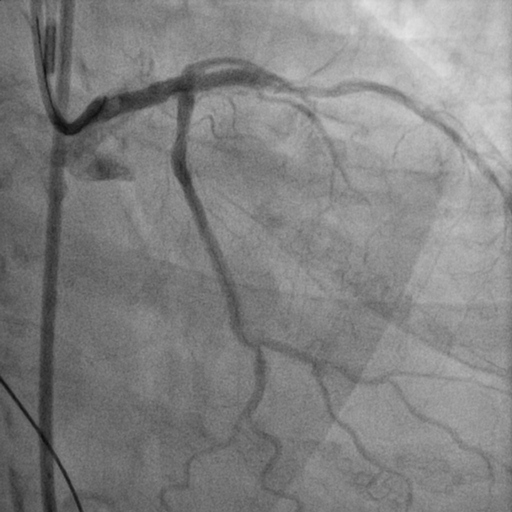
Relevant Catheterization Findings
Left Main : Tight stenosis at distal left main extended to ostial LAD (calcified) Left Anterior Descending : Severe stenosis at osmium (calcified)Left Circumflex : Severe stenosis at ostiumRight Coronary Artery : calcified vessel. mild disease at midRCA


Interventional Management
Procedural Step
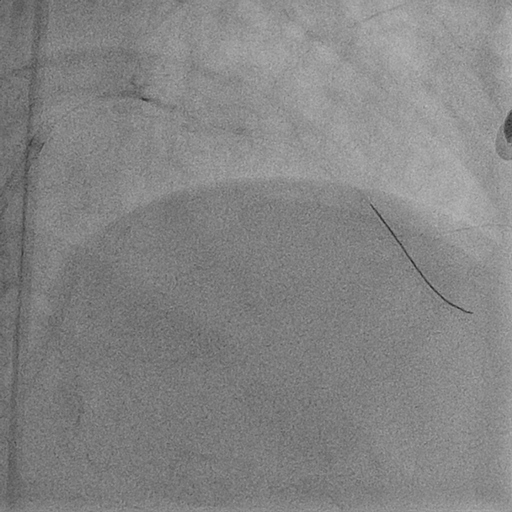
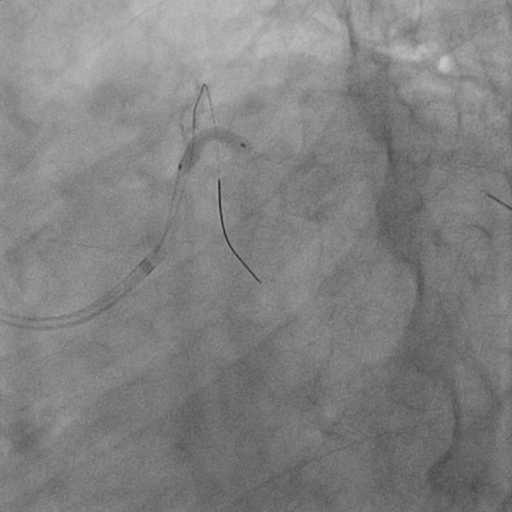
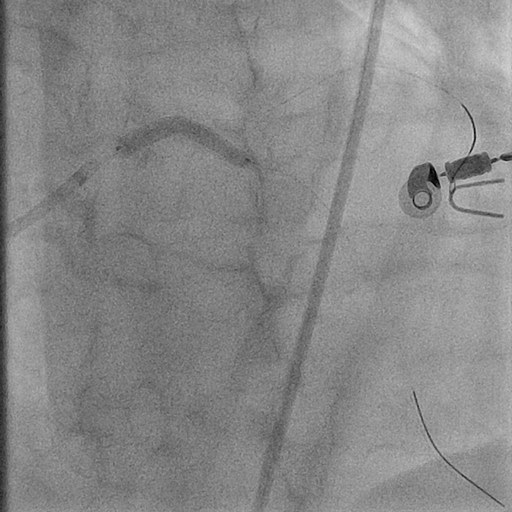
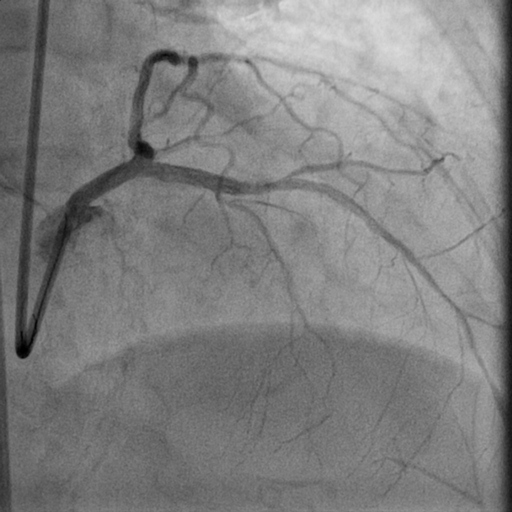
Complex pci with atherectomy and iabp support was planned. Bilateral common femoral artery were cannulated. Guiding catheter ebu 3.0/7fr was engaged to left main and lesion was prepared with semi-compliant (sc) balloon 1.5/15mm at 14 atm as microcatheter could not pass through the lesion. Subsequently runthrough floppy wire was exchanged to viper wire via finecross microcatheter. Orbital diamondback atherectomy at distal lm to lad was performed at 120k rpm. Run-through floppy and sion blue wire were placed at lad and lcx followed by predilatation of lad with non-compliant balloon 3.0/15mm at 18 atm and ostial lcx at 8atm. We decided to go with hybrid approach by performing dcb at the ostial lcx with sequent please 3.0/15mm 30sec (x2) and des ultimaster 3.5/33 from ostium of lm to proximal lad. Stent was postdilated further with 3.75/12mm at 16 atm. Patient was discharged from hospital after 2 days without complication.

 2. OAS.avi
2. OAS.avi
Case Summary
There are varying strategies for distal left main bifurcation intervention with various outcome. To a greater extent the procedure becomes more complex if there is presence of heavily calcified plaque. We demonstrated a hybrid approach with dcb at side branch followed by des at distal left main to main branch after orbital atherectomy.