
CASE20210828_002
Successful Retrieval of Dislodged Non-Inflated Coronary Stent: Where Micro Snare and Stent Broke
By
Presenter
Dileep Kumar Tiwari
Authors
1
Affiliation
, India1
Complications - Complications
Successful Retrieval of Dislodged Non-Inflated Coronary Stent: Where Micro Snare and Stent Broke
1
, India1
Clinical Information
Patient initials or Identifier Number
Saini
Relevant Clinical History and Physical Exam
This is 65 years old gentleman who was a known case of hypertension and diabetes mellitus. He had history of old anterior wall myocardial infarction (AWMI) in 2004 and had severe Left Ventricular (LV) dysfunction (LVEF 35%). He was on regular treatment. This time he was admitted with acute left ventricular failure (LVF). ECG showed QS pattern in lead V1-V4. 2D Echo revealed scarred and akinetic LAD territory and LVEF dropped to 20%.
Relevant Test Results Prior to Catheterization
His serum creatinine level was initially rose from 1.3 to 2.2 mg/dL but after stabilisation it again came down to 1.28 mg/dL. All other lab parameters remained with in normal limits. At this stage coronary angiography planned.
Relevant Catheterization Findings
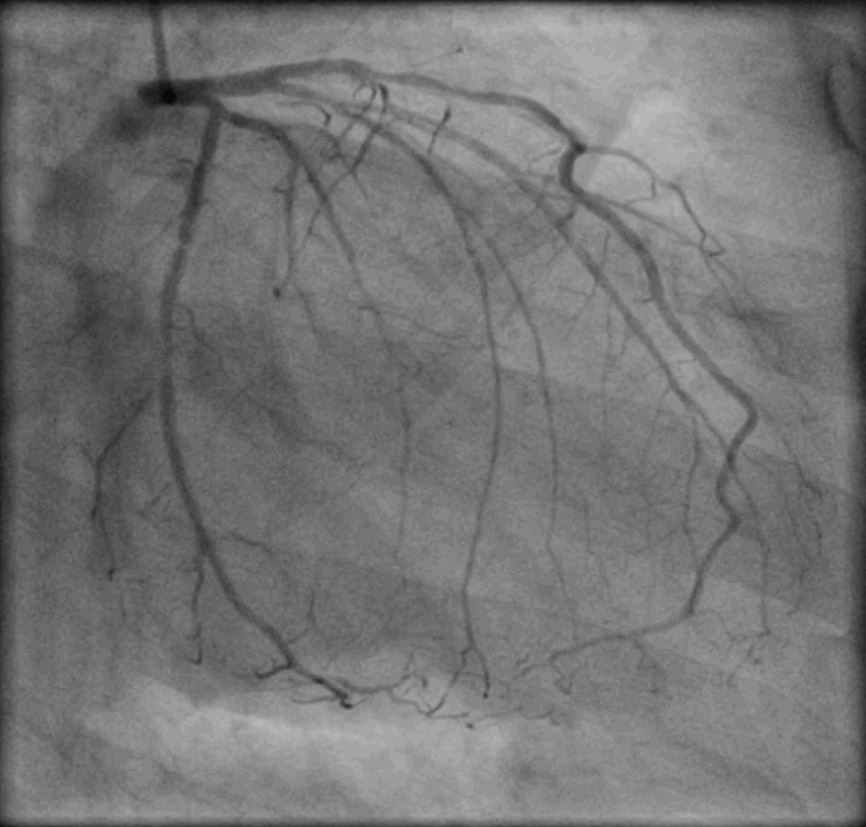
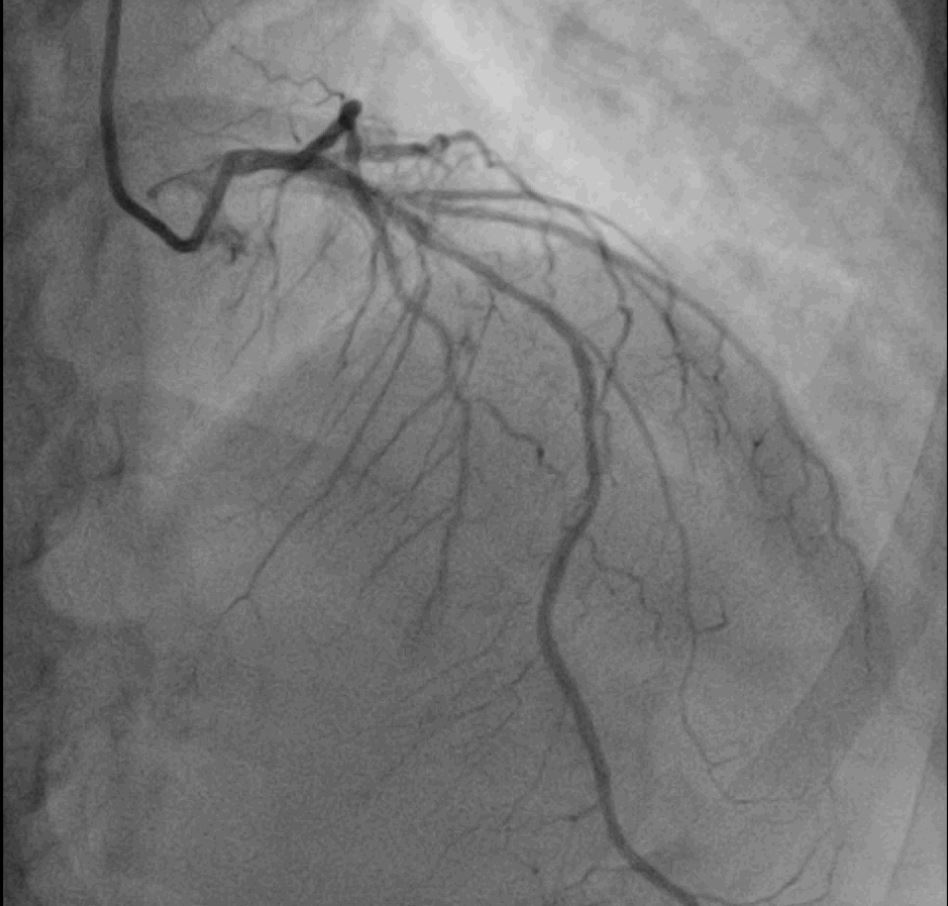
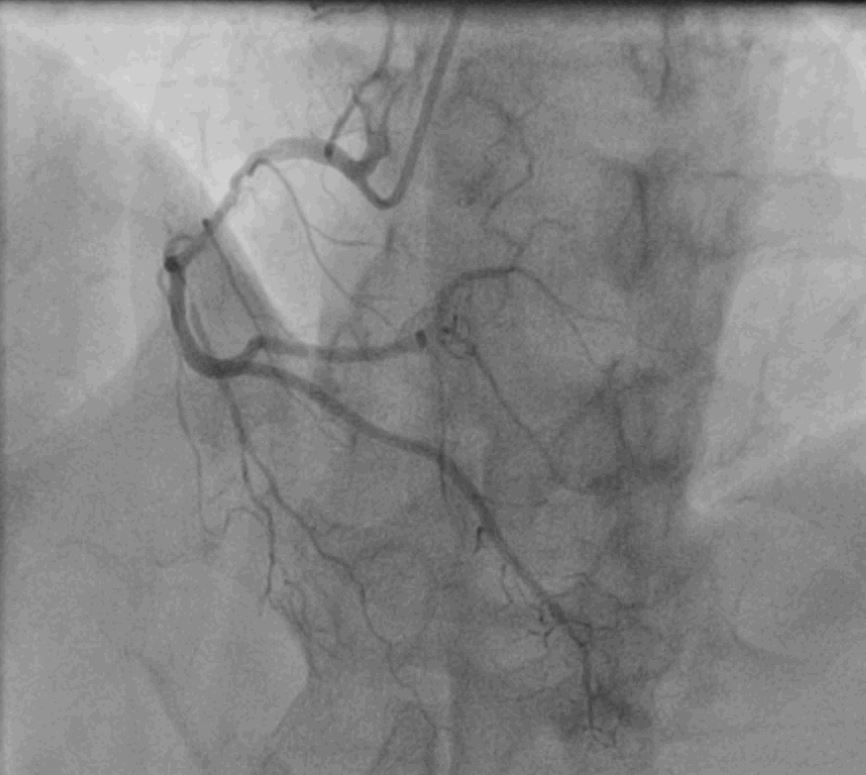
After stabilisation and taking proper written informed consent patient underwent coronary angiography through right radial approach, which revealed calcified Triple Vessel Disease (TVD). with critical LCx and RCA disease. In view of scarred and akinetic LAD territory and marginally raised serum creatinine level PCI to LCx and RCA planned in staged manner.
 1_mpeg4.mp4
1_mpeg4.mp4
2_mpeg4.mp4
5_mpeg4.mp4
Interventional Management
Procedural Step
During PCI of LCx, the left main was hooked with Extra Back Up (EBU) 3.0, 6F’ guiding catheter and lesion was crossed with Rinato guidewire. Lesion was sequentially pre-dilated with 1.5 x 10 mm and 2.0 x 10 mm semi compliant balloon and then 2.5 x 8 mm non-compliant balloon, which was crossed with the help of Guideliner V3, 5.5 F'. While deploying the stent (Ultimaster, Terumo, 2.5 x 38 mm), it got dislodged on manipulation in deflated form. Part of the deflated stent was still inside the guideliner and over the guidewire so proximal part of the stent was picked up by 4 mm snare and while pulling out the stent the snare got broken leaving the stretched portion of proximal stent hanging in ascending aorta. So we took another 20 mm snare system and picked the stent in ascending aorta but during taking it out, the stent broke off in two parts. Distal portion still remained stuck inside the LCx. Part of stretched stent was still hanging in ascending aorta, therefore the whole process with 20 mm snare system was repeated and while applying the pulling pressure, we asked the patient to cough simultaneously. ultimately the remaining part of stent came out successfully leaving no obvious injury or dissection to LM or LCx.

10_mpeg4.mp4
14_mpeg4.mp4
18_mpeg4.mp4
Case Summary
Complications are part and parcel of coronary interventions but successful bailout without doing any harm to the patient is satisfying. Better lesion assessment and use of intravascular lithotripsy (IVL) or Rota ablation could have avoided the complication. Ultimately persistent efforts with a right strategy in right direction is the key to success.