
CASE20210827_002
Rotational Atherectomy in a Heavily Calcified, Balloon Undilatable Left Anterior Descending Artery Chronic Total Occlusion
By , , ,
Presenter
Hou Tee Lu
Authors
1, 1, 1, 1
Affiliation
, Malaysia1
Complex PCI - Calcified Lesion
Rotational Atherectomy in a Heavily Calcified, Balloon Undilatable Left Anterior Descending Artery Chronic Total Occlusion
1, 1, 1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
CCC
Relevant Clinical History and Physical Exam
A 67-year-old male presented with frequent angina on exertion for 1 month. Past medical history included diabetes mellitus, hypertension, morbid obesity (BMI: 43), benign prostatic hypertrophy, gouty arthritis and sleep apnoea syndrome. History of PCI (2013) on mid LAD by a EES 2.5x12mm. Non-smoker. The heart rate was 80/min and blood BP was 140/90 mmHg. He is on cardiprin, Exforge, Galvus-metformin, atrovastatin, bisoprolol and doxazosin.
Relevant Test Results Prior to Catheterization
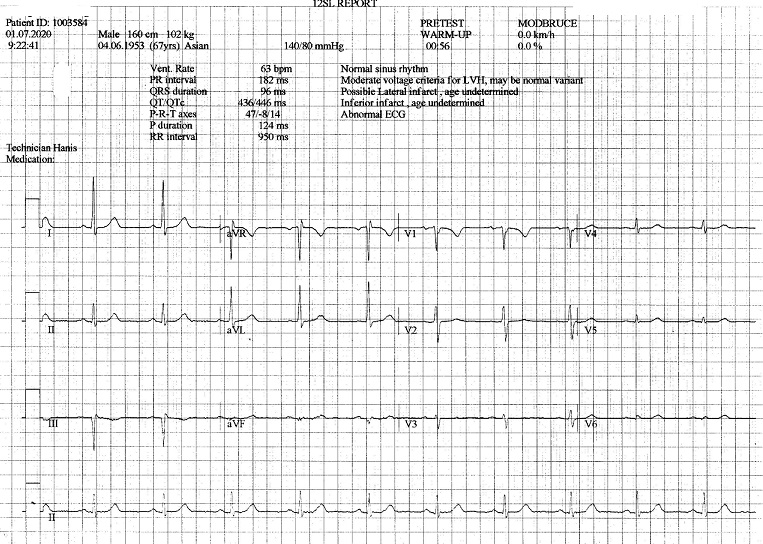
The ECG wasnormal. Troponin T was negative. The exercise stress test was inconclusive,terminated due to fatigue. The echocardiography showed EF of 70%, normal valvesand chambers size. CXR was normal. Blood investigations: Hb: 12.8 g/dL,creatinine: 117 µmol/L, total cholesterol: 3.3 mmol/L and LDL: 1.6 mmol/L, andHbA1c 6.2%.
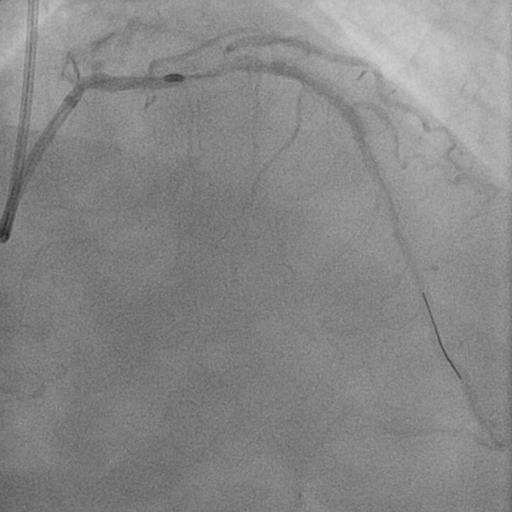
Relevant Catheterization Findings
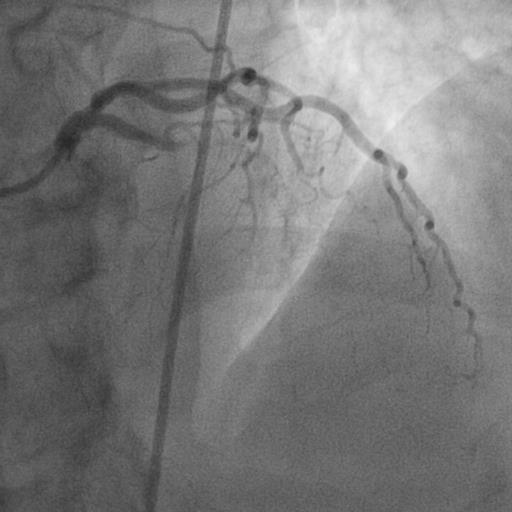
CoronaryAngiographyTransfemoralapproach.1. Normal LMT 2. Proximal LAD 100% occlusion (Chronic totalocclusion), severely calcified proximal LAD and ISR mid LAD 3. LCX artery minordisease (recessive) 4. Mid RCA 60-70%%stenosis- small tortuous collateral from PDA to septal colleteral Option of CABGversus complex PCI explained. Patient and family members declined CABG, agreedfor complex PCI.


Interventional Management
Procedural Step
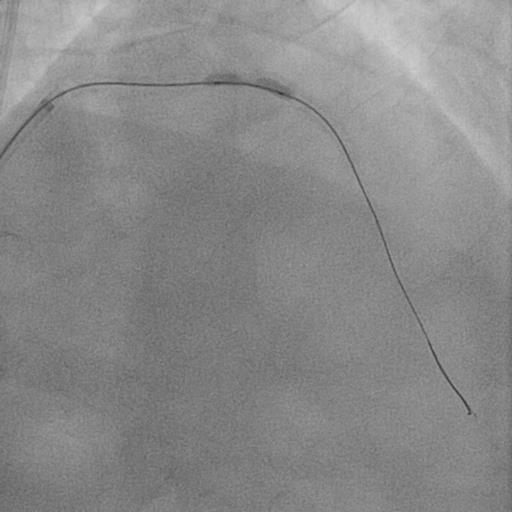
Right and leftfemoral arteries access. An EBU 3.5 (7Fr)GC was used to engage LMT. The RCA was engaged with JR 4.0. Antegrade approachwith Finecross MC, and Fielder XTR wire. XTR was escalated to GAIA 2ndand successfully wired into distal true lumen. However, Finecross MC failed toadvance further for wire exchange due to calcification. The CTO was predilated1.25x10mm compliance balloon. GAIA 2nd was exchanged with aRunthrough floppy wire. Rotational atherectomy (RA) (1.25 mm burr at 180,000rpm for 5 runs) was done on LAD lesion. Then, balloon angioplasty was done usingNC balloon 2.0x8mm, and 2.75x15mm. TIMI 3 flow restored but the proximal LADlesion was severely calcified resistant to balloon dilatation. The use of NC3.0x15mm, NC 3.5x12mm (22 atm), and Scorflex NC 3.5x10mm, and buddy wiretechnique failed to dilate the lesion. Decisionwas made to upsize the Rota burr to 1.75mm. After Rotablation, repeatpredilatation with NC 3.5x10mm resulted in balloon ruptured and successfullycracked the calcified plaque. No dissection or vessel perforation. Lesions weretreated with EES 2.75x38mm, EES 3.0x38mm. The stents were post dilated with NC3.0x15mm balloon. Procedure was successfully. Unfortunately, left femoral puncturesite was complicated by hematoma and a left AV fistula, managed conservatively. Patient was discharged after 5 days of hospitalization.

Case Summary
Treating calcified, balloon undilatable lesion is challenging and potentially risky. Careful planning and implementation of a stepwise, algorithmic approach can help optimize outcomes. For complex PCI, attention should be paid to femoral puncture site to avoid complications such as hematoma, pseudoaneurysm or AV fistula.