
CASE20210827_001
A Challenging Case of Recalcitrant Coronary Calcium
By ,
Presenter
F. Aaysha Cader
Authors
1, 1
Affiliation
, Bangladesh1
Complex PCI - Calcified Lesion
A Challenging Case of Recalcitrant Coronary Calcium
1, 1
, Bangladesh1
Clinical Information
Patient initials or Identifier Number
C1
Relevant Clinical History and Physical Exam
A 74 year-old frail gentleman withmultiple co-morbidities (diabetes, hypertension, dyslipidaemia,BEP) presented with CCS class III-IV angina despite guideline directed medicaltherapy. HE had stable haemodynamics on admission.
Relevant Test Results Prior to Catheterization
ECG showed mild ST-T changes in inferior leads. Echo showed a preserved ejection fraction of 65%.
Relevant Catheterization Findings
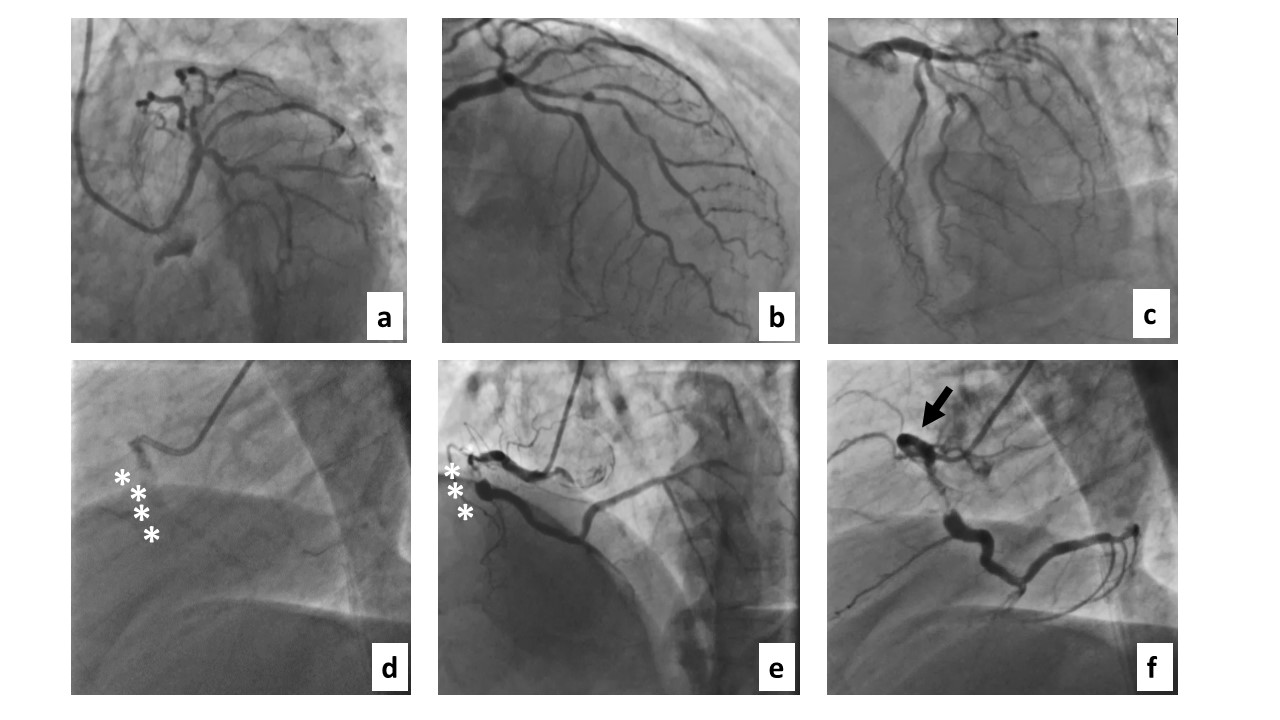
Coronary angiography done transradially revealed significantly diseased Diagonal, distal Obtuse Marginal (OM) & severely calcified right coronary artery (RCA).
 2.avi
2.avi
4.avi
8.avi
9.avi
Interventional Management
Procedural Step
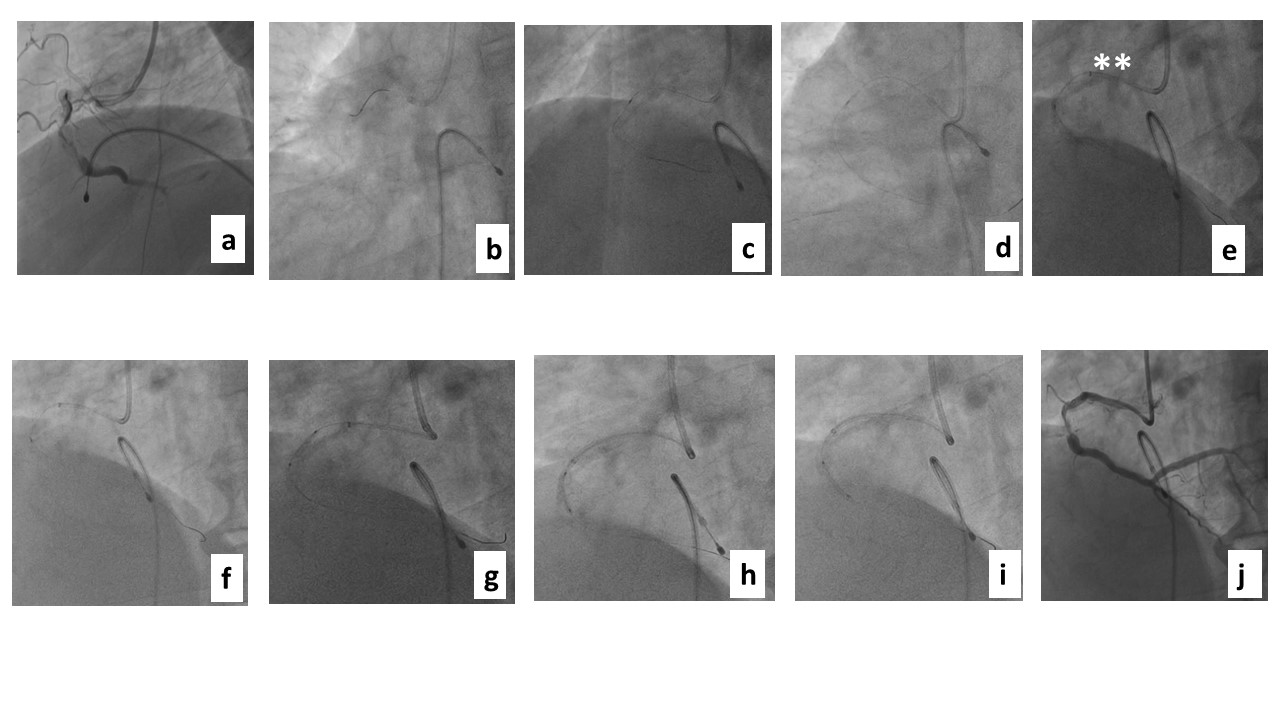
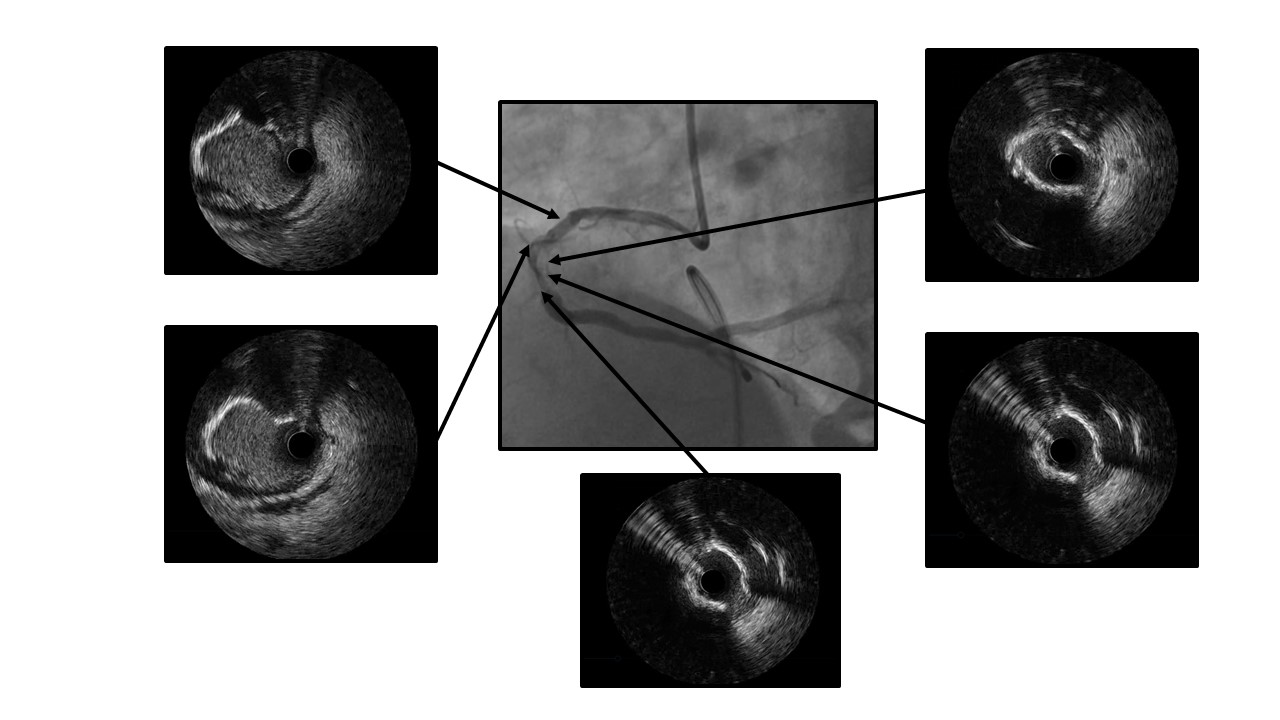
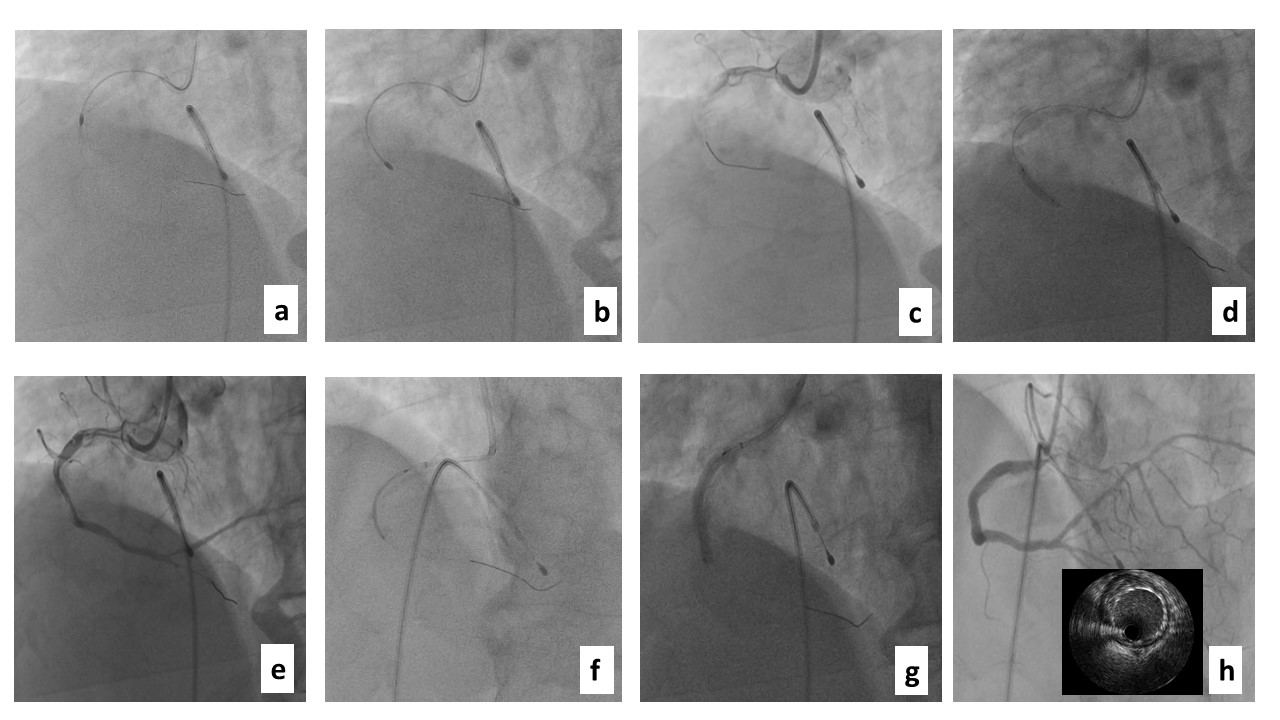
PCI to RCA was done aselective procedure. Temporary pacing wire (TPW) was placed. Using JR 3.6 6French guide, PT2 moderate support polymer tip hydrophilicwire (Boston Scientific Corp, Natick, Massachusetts, USA with1.25x5 m balloon support was used for wiring, which was difficult to wire dueto severe tortuosity and calcification. It ultimately crossed with the supportof Finecross microcatheter, which did not cross. 1.25x5 mm balloonpartially crossed, grenadoplasty was done, with another 1.5x10 mm balloon (Fig 2). IVUSshowed severe concentric 360 degree “napkin ring” calcification (Fig 3). 4 runs ofrotational atherectomy were performed with 1.5 mm burr at 160,000 rpm (Fig4). Thepatient became entirely dependent on temporary pacing then. Distal embolization of debris led to no reflow. After further lesionpreparation the lesion was stented by 3.5x38 mm Everolimus eluting stent (EES),with good angiographic and imaging result
Case Summary
PCI of severely calcified tortuousis challenging especially if balloon-uncrossable. Multiple techniquesincluding grenadoplasty, upscaling of non-compliant balloons, rotationalatherectomy and the use of guide extension, temporary pacing wire andintravascular ultrasound (IVUS) were necessary for successful stent deployment.