
CASE20210823_003
Complete Revascularization in High Bleeding Risk Patient
By ,
Presenter
Nay Thu Win
Authors
1, 2
Affiliation
, United Kingdom1, , Malaysia2
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Complete Revascularization in High Bleeding Risk Patient
1, 2
, United Kingdom1, , Malaysia2
Clinical Information
Patient initials or Identifier Number
WH
Relevant Clinical History and Physical Exam
A 63 yr old gentleman who has diabetes mellitus, hypertension, dyslipidaemia and recurrent bilateral lacunar stroke 3 years ago, presented with chest pain. Cardiac enzyme are raised and ECG showed right bundle branch block with T inversion at V2 and V3.
Relevant Test Results Prior to Catheterization
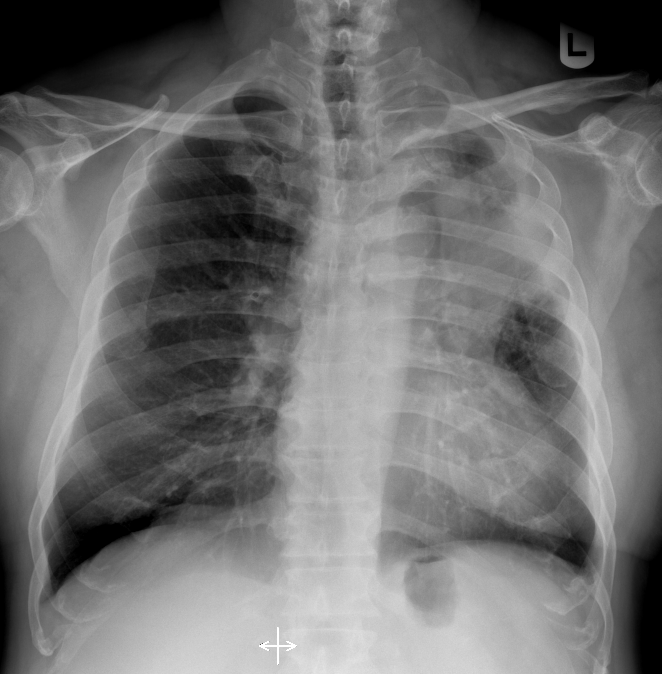
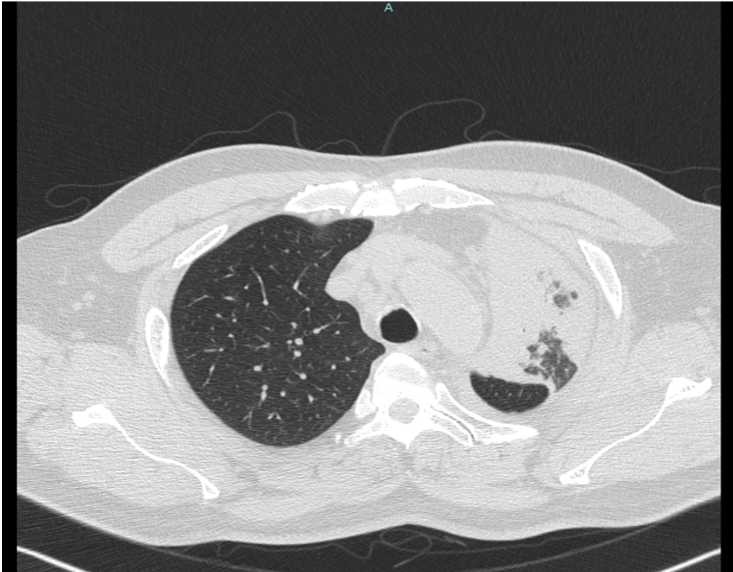
Cardiac enzymes are raised. Renal function, liver functionand full blood counts were normal. Chest X-Ray revealed left upper lobeconsolidation. HRCT showed LUL consolidation with calcification foci within centre of consolidated lungs. CT guided biopsy by respiratory team revealed adenocarcinoma of lungOncologist suggested for revascularization prior to chemotherapy.
Relevant Catheterization Findings
Coronary angiogram revealed moderate left main disease (30%), severe stenosis with calcification of LAD from proximal to distal LAD and severe stenosis of LCX from ostial to distal LCX and severe stenosis at distal RCA. Multidisciplinary team meeting decided that he is not a suitable for CABG due to lung malignancy and probable difficulty in extubation after operation. We explained the risk and benefits of high risk PCI and consented.
 CRa.mpg
CRa.mpg
caud.mpg
rca cra.mpg
Interventional Management
Procedural Step
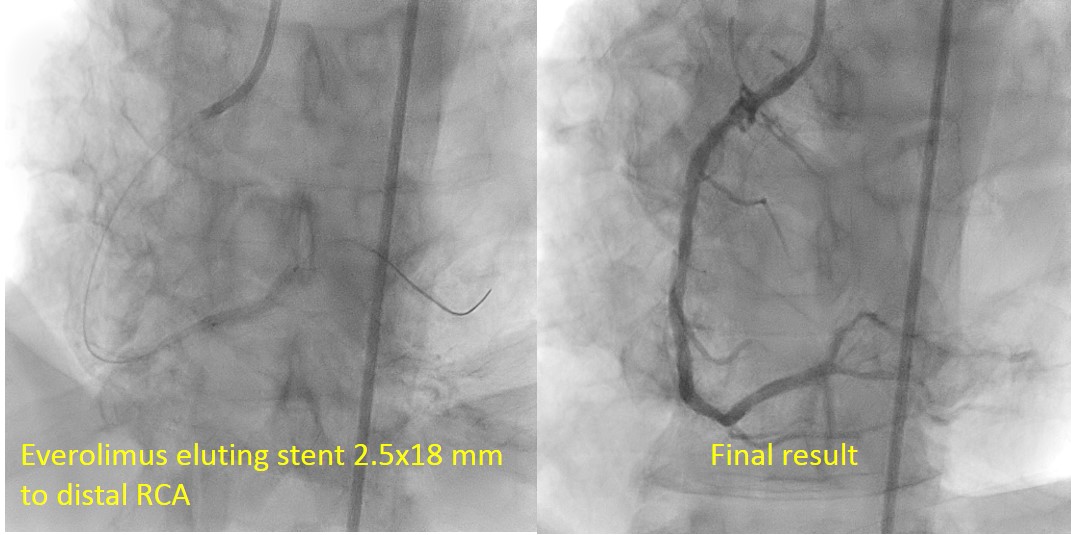
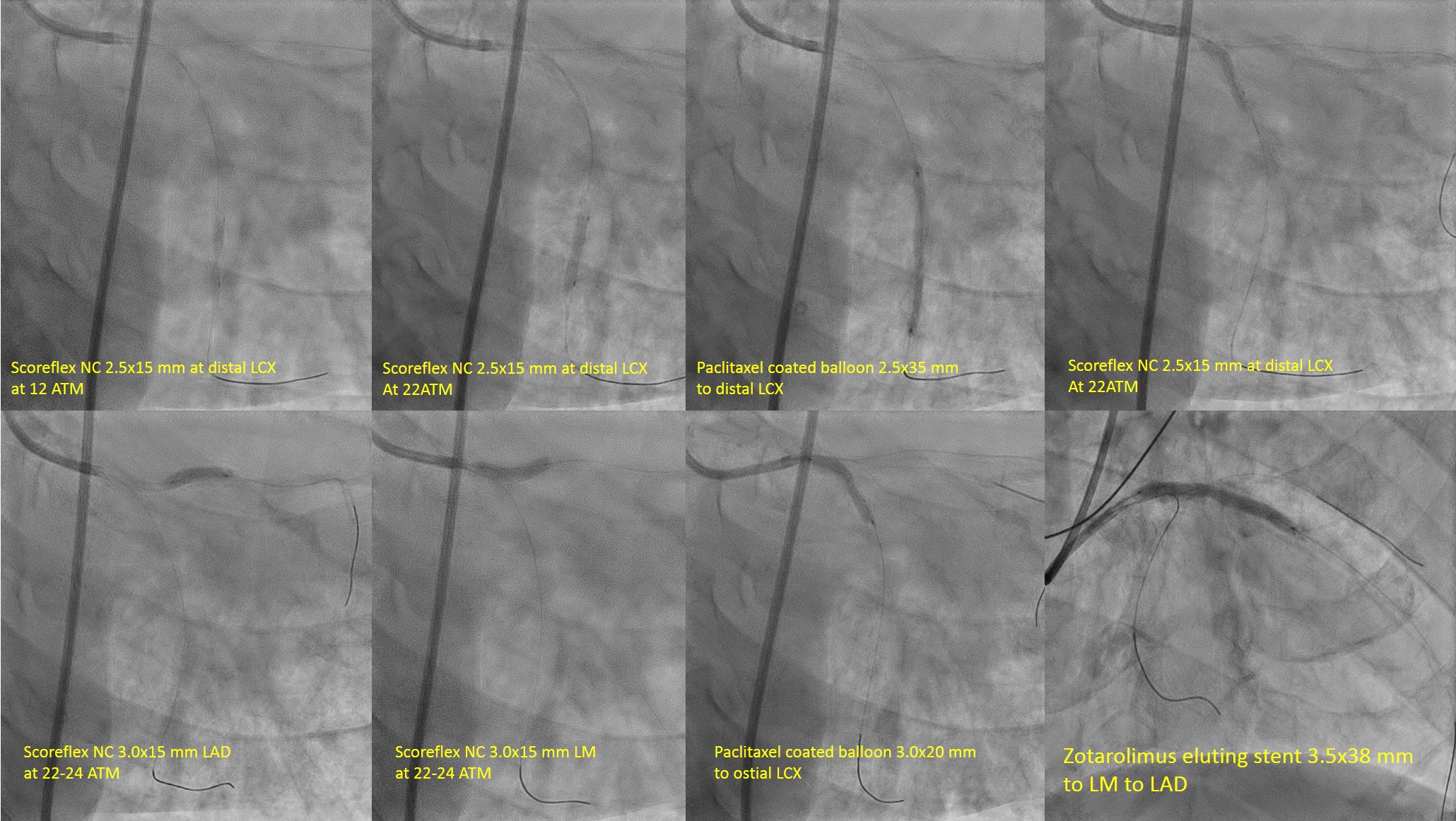
According to ARC HBR criteria, this patient has one major and 2 minor criteria of bleeding. We planned for ccomplete revascularization with provisional one stent strategy for LM bifurcation with DCB in LCX. Firstly, PCI to RCA was undergone with Everolimus Eluting Stent 2.5/18mm. Then, we did stage PCI to LM bifurcation 2 weeks later. EBU 3.5/7F to left main and wired with Run-through floppy to LAD and SION Blue to LCX. LCX was predilated with SCOREPLEX 2.5/15 mm at distal segment at 22-24 ATM. Drug coated balloon with paclitaxel eluting balloon 2.5 x 35 mm at distal to mid circumflex. Then, LAD was predilated with Scoreflex NC 3.0x15 mm at 20 to 24 ATM. 3rd wire to first diagonal and POBA to first diagonal with Wilma 2.0 x25 mm at 12 ATM. Drug coated balloon with paclitaxel eluting balloon 3.0x20 mm at 6ATM in ostial and proximal circumflex. LAD was stented with Resolute Onyx 3.5x38mm at 12ATM. We FLIP-FLOP the diagonal wire to LAD. Proximal optimisation technique (POT) in left main with NC TREK 4.0x8mm at 20 ATM. Patient was discharged with Aspirin and Clopidogrel for one month
final cra.mpg
final caud.mpg
Case Summary
Patient was referred to Oncologist for chemotherapy. During our review HB dropped from 15.2 g/dl to 13.5 g/dl. Hence, he was referred to gastroenterologist for OGDS, which revealed duodenitis. Then, We stopped aspirin and discharge with single anti platelet. clopidogrel. He is doing well during regular follow up. Complex PCI to left main bifurcation was done successfully in HBR patient. Provisional stenting with the short DAPT approved stent in left main -LAD and DCB to LCX achieved a good result.