
CASE20210820_003
A Simple Percutaneous Coronary Intervention May Complicated Unexpectedly - Aorto Coronary Dissection Treated with Non Covered Stent across the Ostium
By ,
Presenter
MOHAMMAD SHAFIQUR RAHMAN PATWARY
Authors
1, 1
Affiliation
, Bangladesh1
Complications - Complications
A Simple Percutaneous Coronary Intervention May Complicated Unexpectedly - Aorto Coronary Dissection Treated with Non Covered Stent across the Ostium
1, 1
, Bangladesh1
Clinical Information
Patient initials or Identifier Number
ID- 103025
Relevant Clinical History and Physical Exam
Mr. X 46 years old gentle man, hypertensive, non-diabetic,smoker presented with
Relevant Test Results Prior to Catheterization
Electrocardiogram showed old myocardial infractioninferior. Echocardiogram showed hypokinetic left ventricular inferiorwall with LVEF 62 %.
Figure1 : ECG shows OMI InferiorFigure2 : Echocardiogramshows normal LA , Aorta and LV diameter with LVEF 62 %Figure3 : Echocardiogram shows normal LV cavity diameters with hypokinetic inferior wall
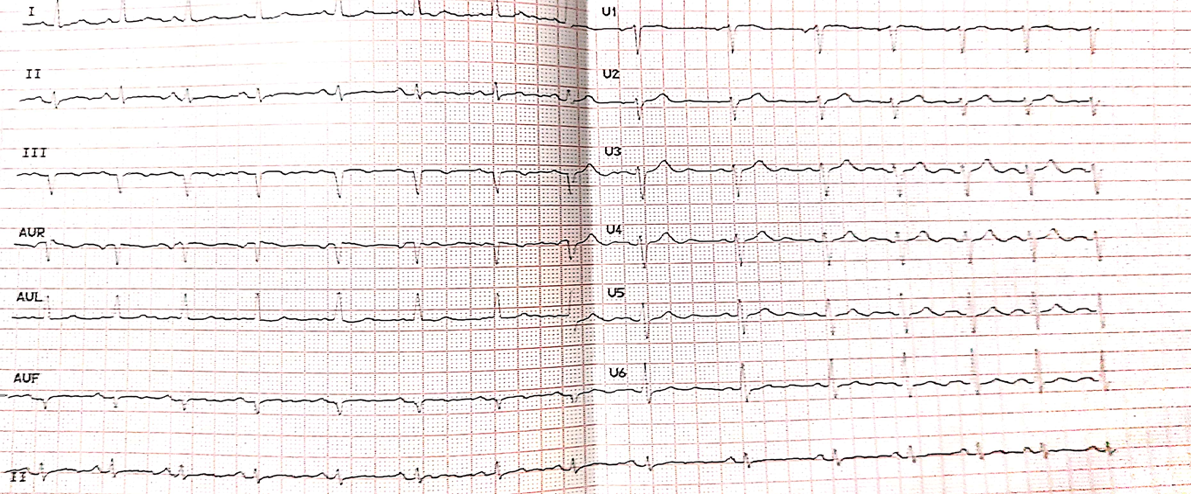
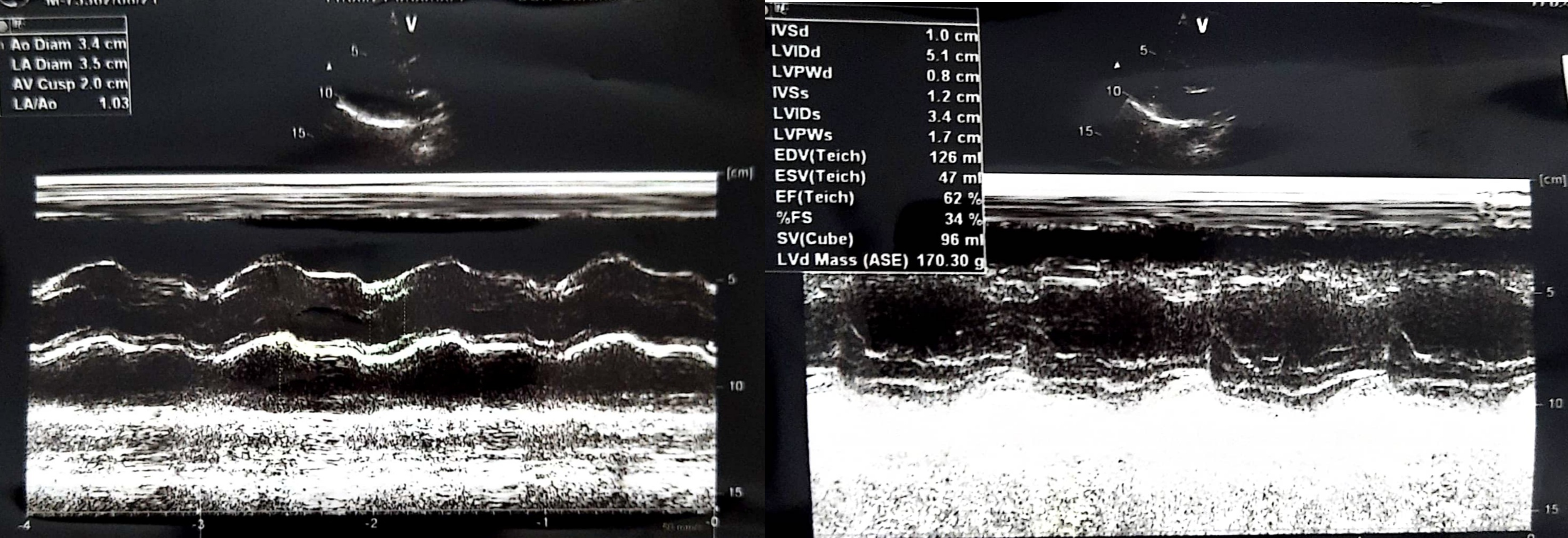
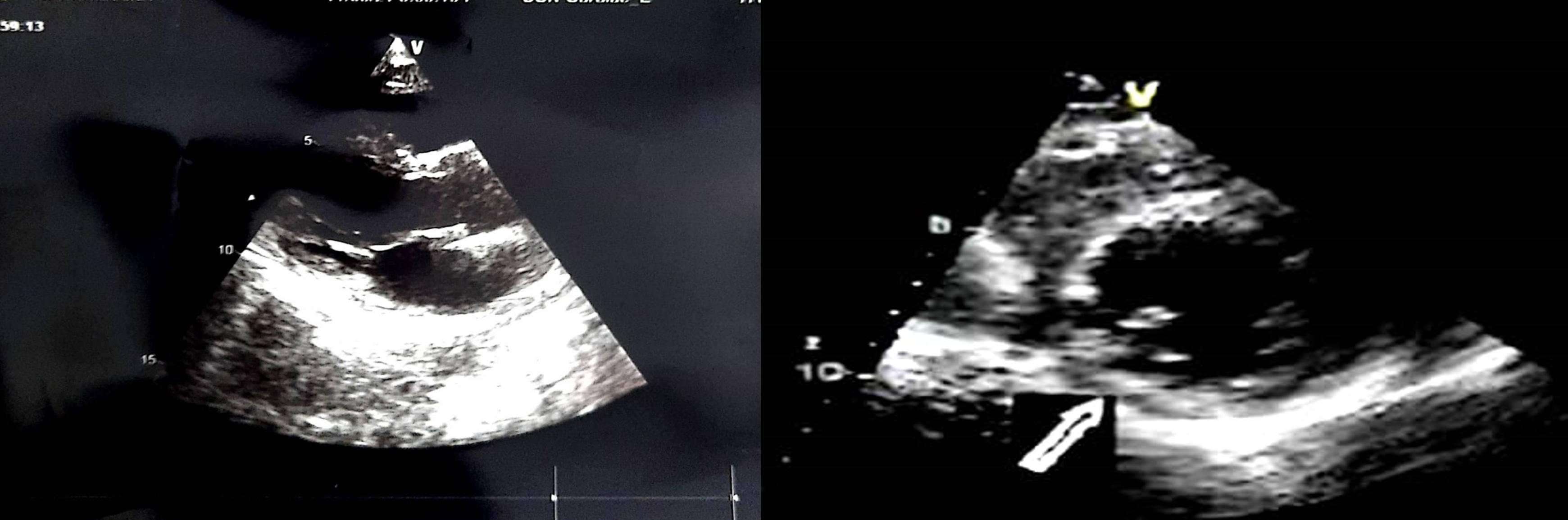
Figure1 : ECG shows OMI InferiorFigure2 : Echocardiogramshows normal LA , Aorta and LV diameter with LVEF 62 %Figure3 : Echocardiogram shows normal LV cavity diameters with hypokinetic inferior wall
Relevant Catheterization Findings
Coronary angiogram through right distal radial artery reveals normal leftmain coronary artery. Left anterior descending artery showed minor plaque inmid part.Left circumflex coronaryartery was non dominant and 30% stenosis in mid OM1.Right coronaryartery dominant vessel with 99% stenosisin proximal part of posterior descending artery.
Video 1 : Coronaryangiogram of right coronary artery showed 99% stenosis in proximal part ofposterior descending artery
 Video1.mp4
Video1.mp4
Video2.mp4
Video3.mp4
Video 1 : Coronaryangiogram of right coronary artery showed 99% stenosis in proximal part ofposterior descending artery
Interventional Management
Procedural Step
6F JR 3.5 Medtronic Launcher Coronary Guide Catheter, USA was used.Terumo Runthrough NS Floppy PTCA guide wire 0.014”(0.36mm), Japan crossed thelesion and parked in the distal part of the PDA . Pre dilatation was done with Maverick2 ™PTCA BalloonCatheter, Boston Scientific, USA 2.0 mm X 12mm semi complaint balloon at 8 atm.
Video 4 : After PDA stenting with ResoluteIntegrity RX Zotarolimus Eluting Coronary 2.25mm X 30 mm stent , dye held up inostium , dissection flap in proximalpart and flow compromised in distal part of RCA. Dissection of RCA also extendinto the ascending aorta creating a type A dissection ( Debakey type II ) ofaorta.
Video4.mp4
Video5.mp4
Video6.mp4
Video 4 : After PDA stenting with ResoluteIntegrity RX Zotarolimus Eluting Coronary 2.25mm X 30 mm stent , dye held up inostium , dissection flap in proximalpart and flow compromised in distal part of RCA. Dissection of RCA also extendinto the ascending aorta creating a type A dissection ( Debakey type II ) ofaorta.
Case Summary
Catheter-induced aorto coronary dissection during Percutaneous CoronaryIntervention is a relatively infrequent, but potentially life-threateningcomplication. Although treatment of ascending aortic dissection may requiresurgical repair, stenting at the origin of the dissection area may besufficient in aorto coronary dissection following Percutaneous CoronaryIntervention. Our patient 64 years hypertensive gentle man presented with oldmyocardial infraction inferior with angina with critical lesion in proximalpart of PDA. During PCI unfortunately simple procedure may turn into morecomplicated scenario involving dissection of whole RCA including ostium andascending aorta creating a type a dissection (Debakey type II) of aorta.