
CASE20210820_001
High Risk PCI of LM Bifurcation with CTO Ostial LCX
By
Presenter
Thanawat Suesat
Authors
1
Affiliation
, Thailand1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
High Risk PCI of LM Bifurcation with CTO Ostial LCX
1
, Thailand1
Clinical Information
Patient initials or Identifier Number
Mrs. N M
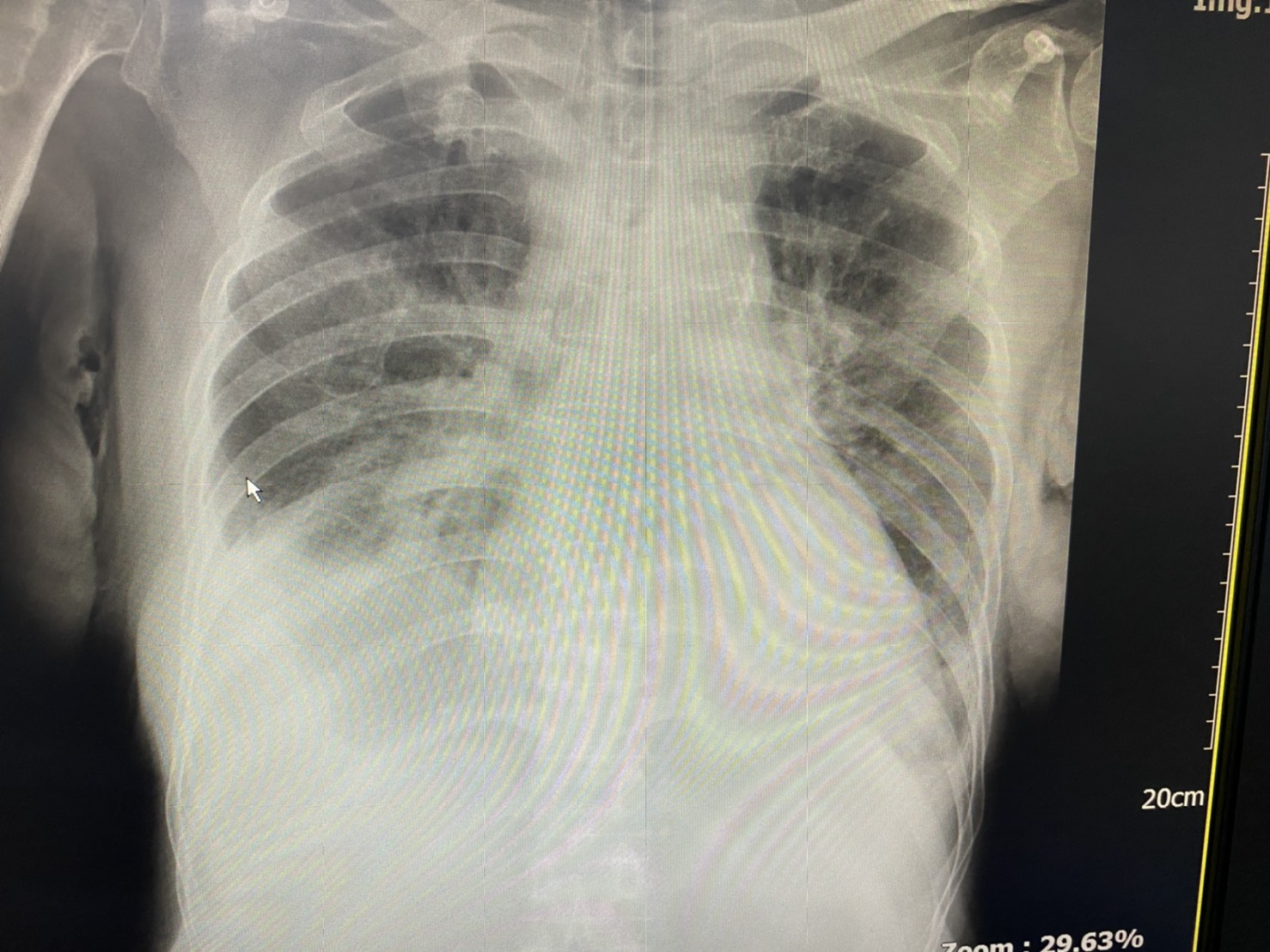
Relevant Clinical History and Physical Exam
chest pain and dyspnea for 1 day
Recurrent CHF 4 times in 6 month ESRD onregular HD 3/week COPD DCM/ ICM EF = 22 % with global hypokinesia , Mild MR ,TR and AR refused to CAG and only medical Rx @ CHF clinic
Recurrent CHF 4 times in 6 month ESRD onregular HD 3/week COPD DCM/ ICM EF = 22 % with global hypokinesia , Mild MR ,TR and AR refused to CAG and only medical Rx @ CHF clinic
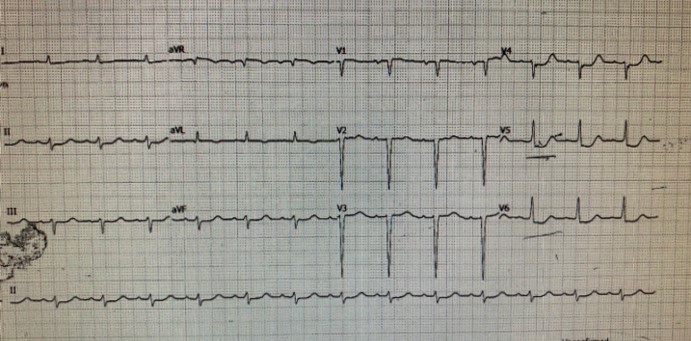
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
LM : calcification ,90 % distal LM stenosis LAD : calcification , 80 % ostial LAD,70 %mid LAD stenosis LCX : calcification , 100 % ostial LCX minimal bridging collateral RCA : non significant stenosis
 1.avi
1.avi
2.avi
3.avi
Interventional Management
Procedural Step
PCI + LM , LAD + LCX (if fail LCX sacrifice of LCX )heavy calcified : Arthrectomy ? Yes (but see from IVUS data ) Temporary pacemaker Hemodyanamic support ? Low LVEF + CHF only IABP available
26.avi
28.avi
30.avi
RFA . 7F EBU 3.5 side hole GD
IABP via LFA , Temp pace vis LFV for hemodynamic supported
Predilated with small balloon 2.0 x15
exchange to rota floppy Rotablator 1.5 burr 180,000 rpm x 3 run , follow by NSE alpha scoring balloon 3.0 x 13 @ 14atm
Try to open LCX ,Pilot 50 + Finecross failed Pilot 200 + Crusade type R double lumen MC Injection from MC ,Seqential dilated with
Balloon SC 1.5 x 15 ,Balloon SC 2.0 x 15 ,Balloon NC 2.5 x 15
Stent mid LAD ZES 3.0 x 18 overlapped position with ZES 3.5 x 24
Position LCX stent and deployed
mini crush technique .position LCX stent with
ZES 3.0 x 14 with Guidezilla guide extension
Mini crush with LM-LAD stent , rewire and kissing
POT NC with NC 4.0 x 8 and final angiogram
Case Summary
contrast 100 ml
80 minutes procedure time
off IABP 6 hr after PCI
Off ET tube 24 hr later
D/C 3 days after PCI
Improve symptoms , No cheat pain
Follow up regular at CHF clinic without readmission
for 6 months
Improve LVEF to 42 %
PCI with LM bifurcation + CTO ostial LCX is very complex in high risk patient