
CASE20210818_002
A Case of Double Jeopardy
By ,
Presenter
F. Aaysha Cader
Authors
1, 1
Affiliation
, Bangladesh1
Complex PCI - Multi-Vessel Disease
A Case of Double Jeopardy
1, 1
, Bangladesh1
Clinical Information
Patient initials or Identifier Number
DJ
Relevant Clinical History and Physical Exam
A 34 year-old hypertensive dyslipidaemic malepresented with chest pain for 6 hours to another centre, where his ECG showedinferior STEMI and he was thrombolysed withTenecteplase. He was later referred toour centre with CCS Class III-IV angina of approximately 36 hours.
Relevant Test Results Prior to Catheterization
ECG showed Q in inferior leads with ST-T changes in anterior leads. Echo showed an EF~50%.
Relevant Catheterization Findings
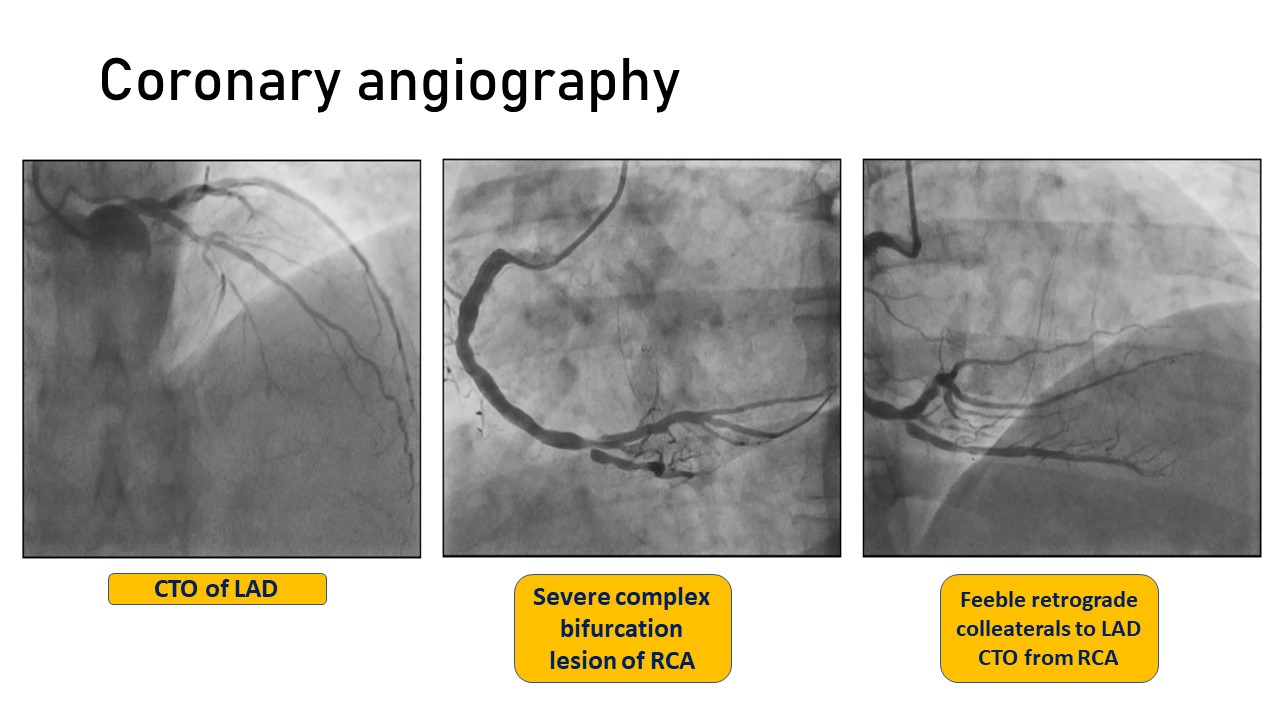
Emergent coronary angiography revealed a CTO of LAD from its mid part with Grade II ipsilateral epicardial collaterals from the large diagonal, i.e. multivessel disease in setting of STEMI. This is a case of “Double jeopardy” i.e. the concurrent presence of a non-IRA CTO in a patient of acute MI, where the newly occlusive IRA may supply collaterals to CTO, resulting in larger area of subtended myocardium. In our case, the
Interventional Management
Procedural Step
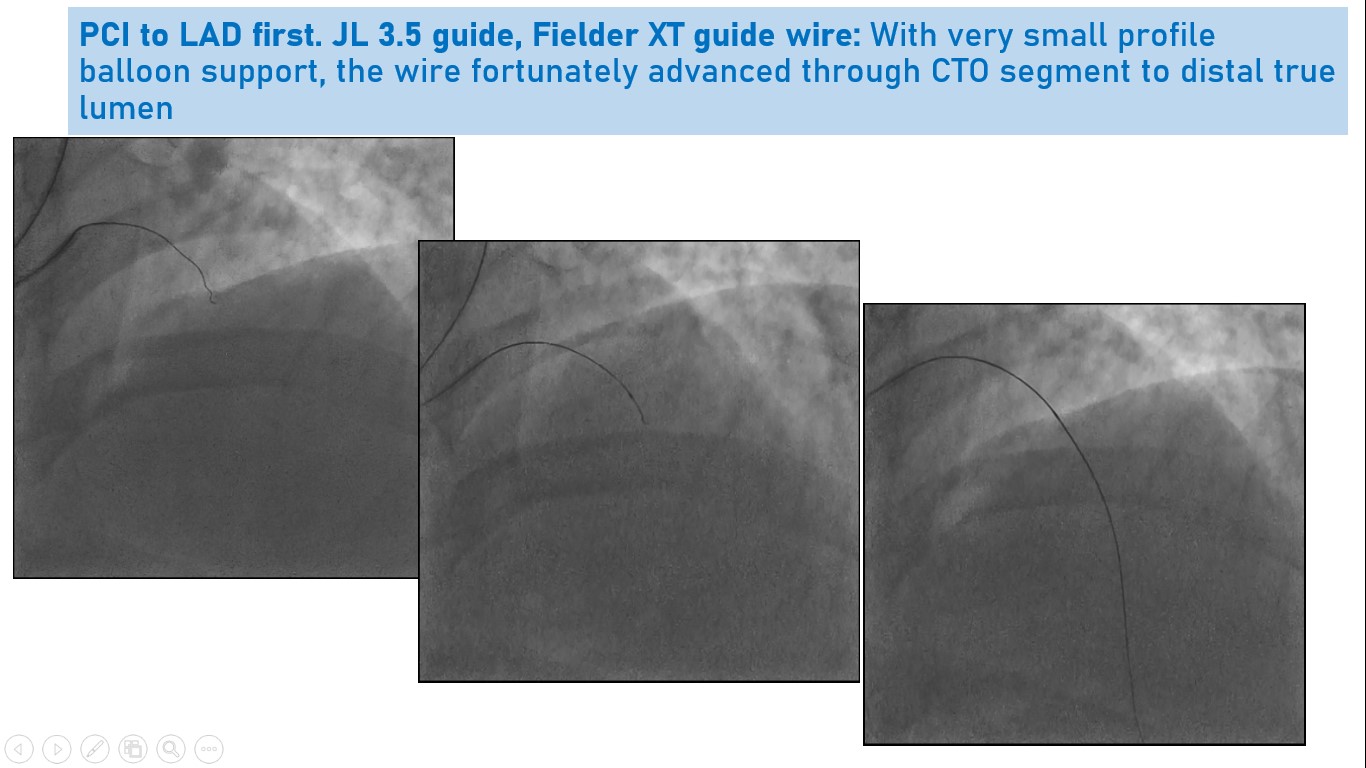
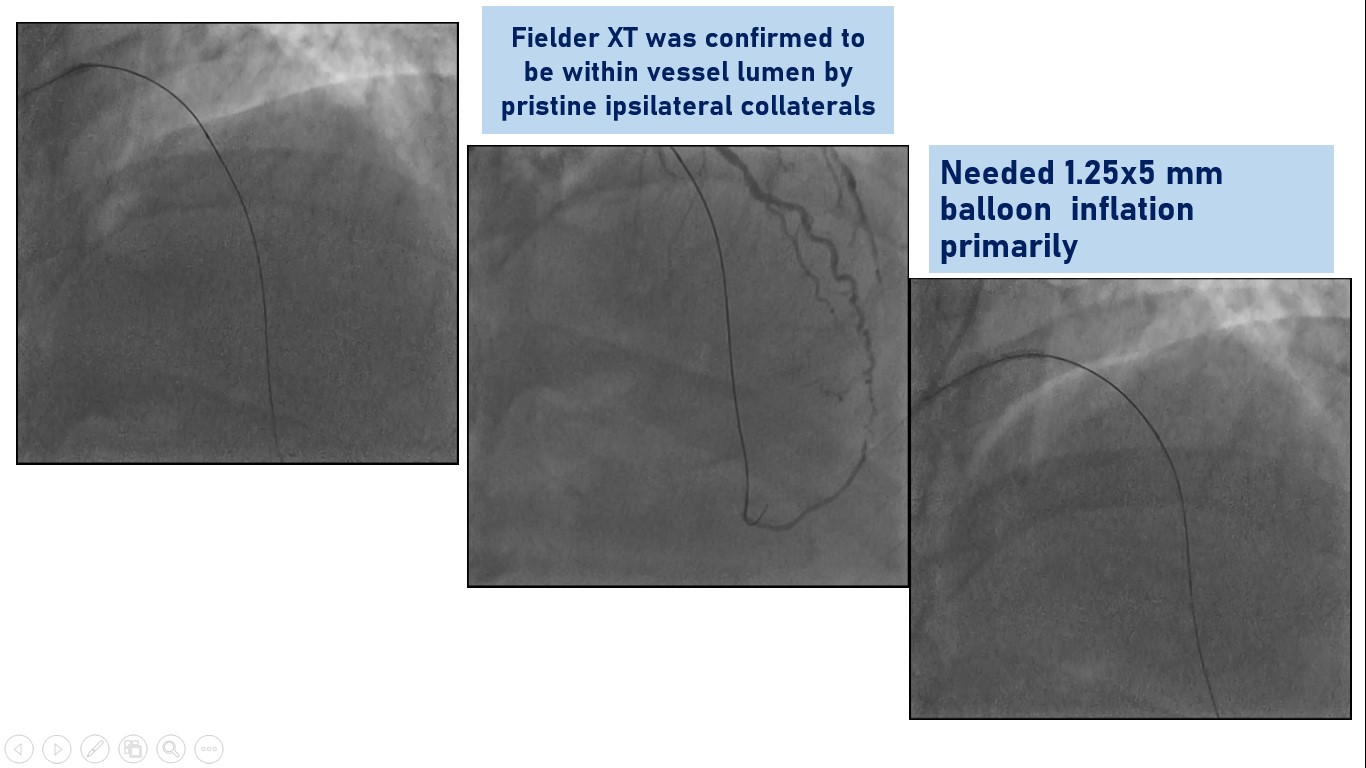
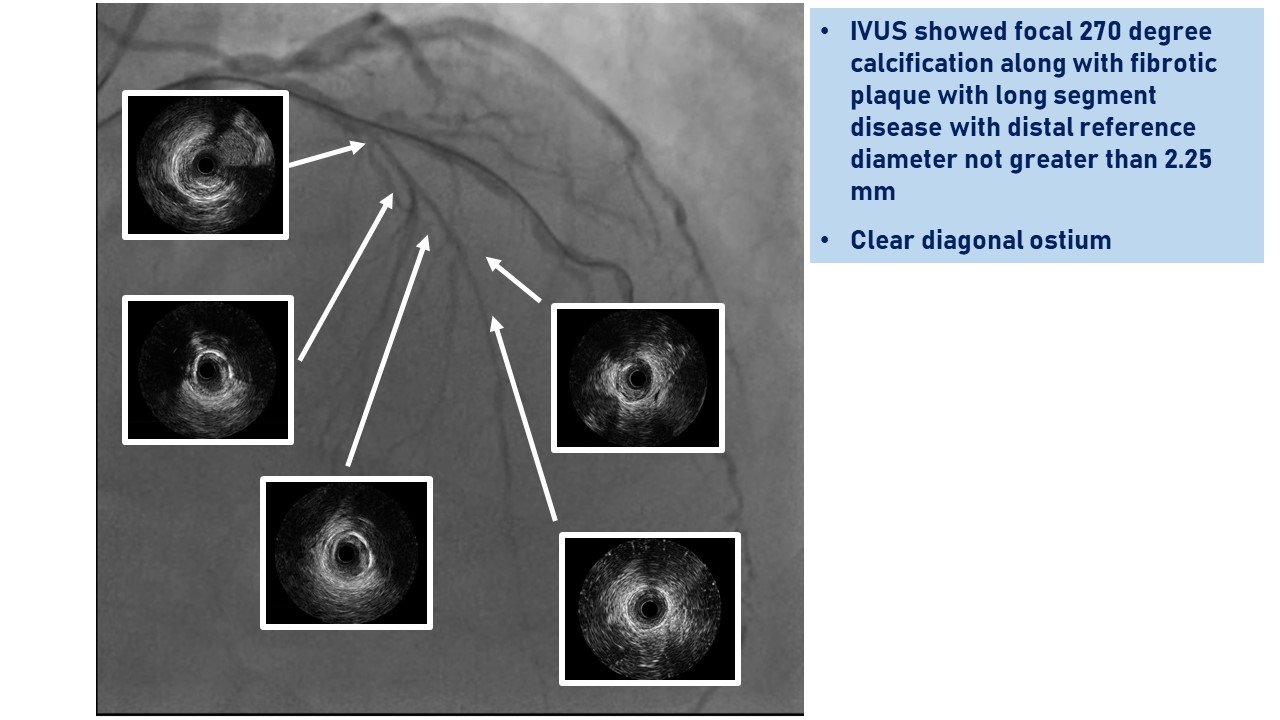
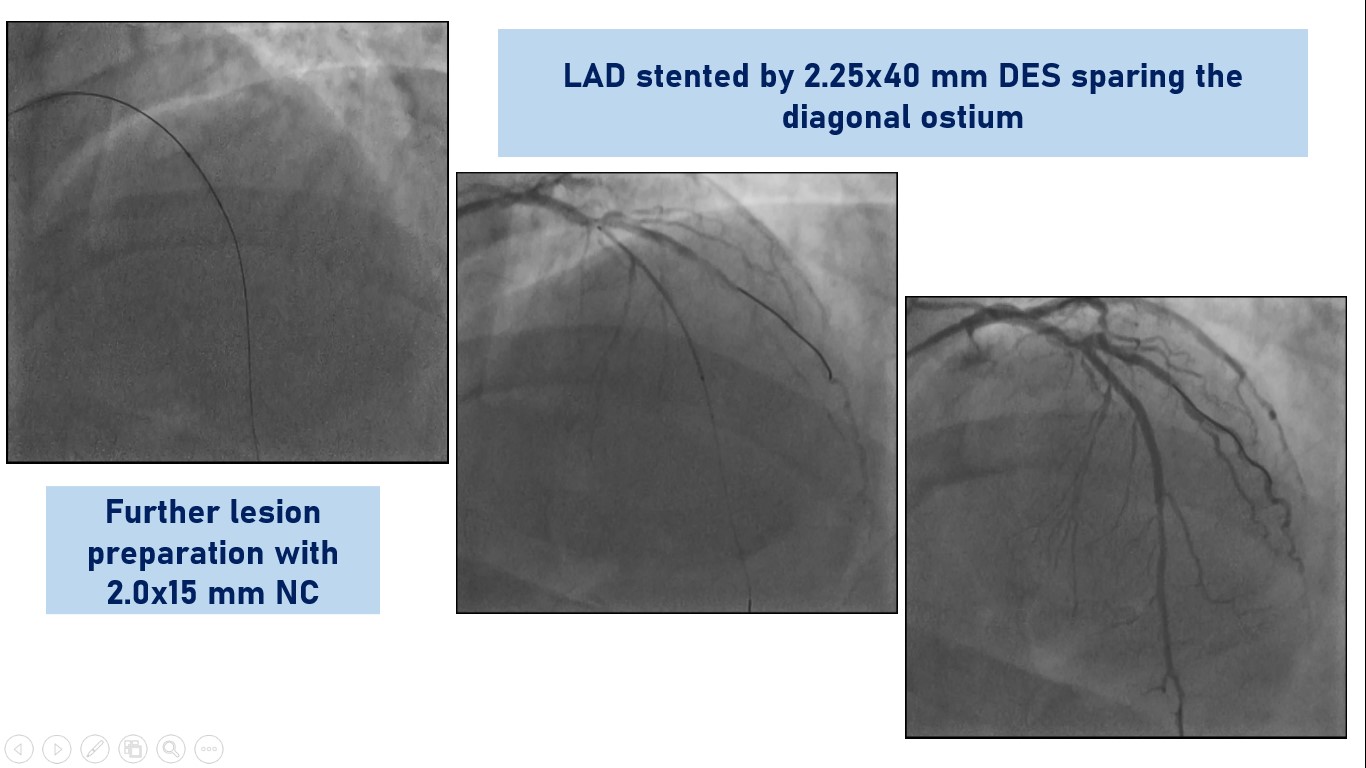
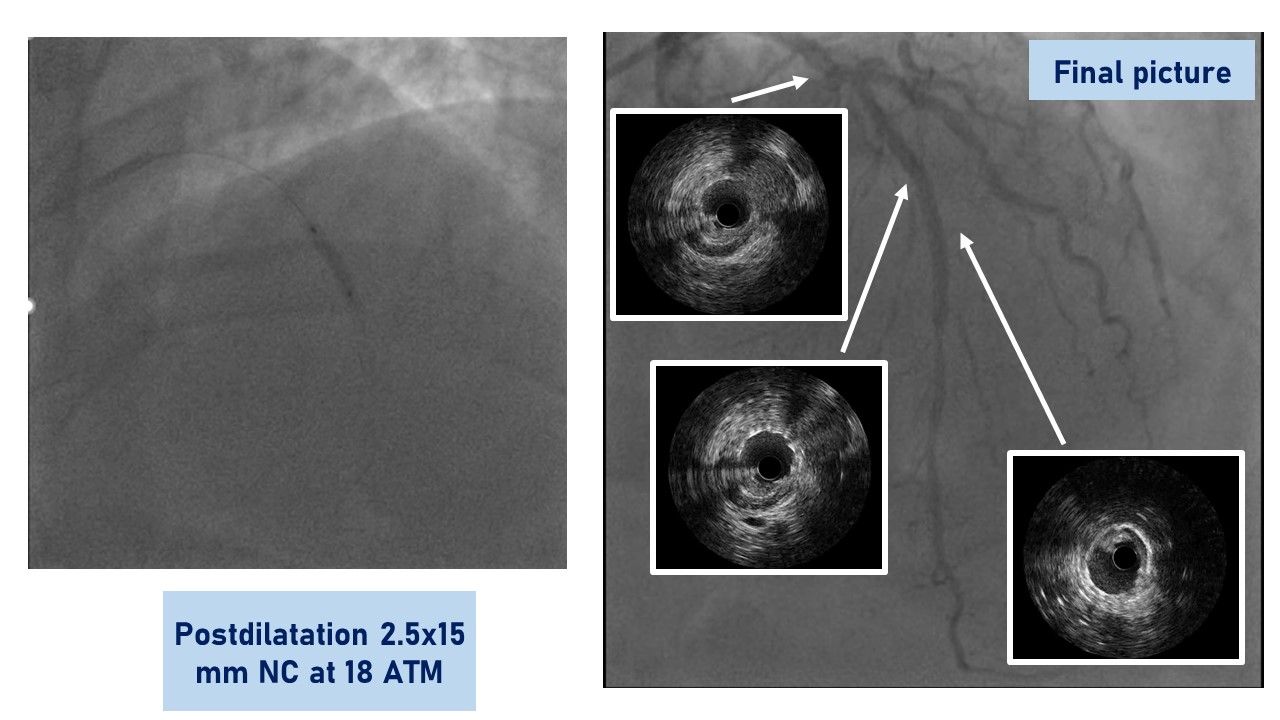
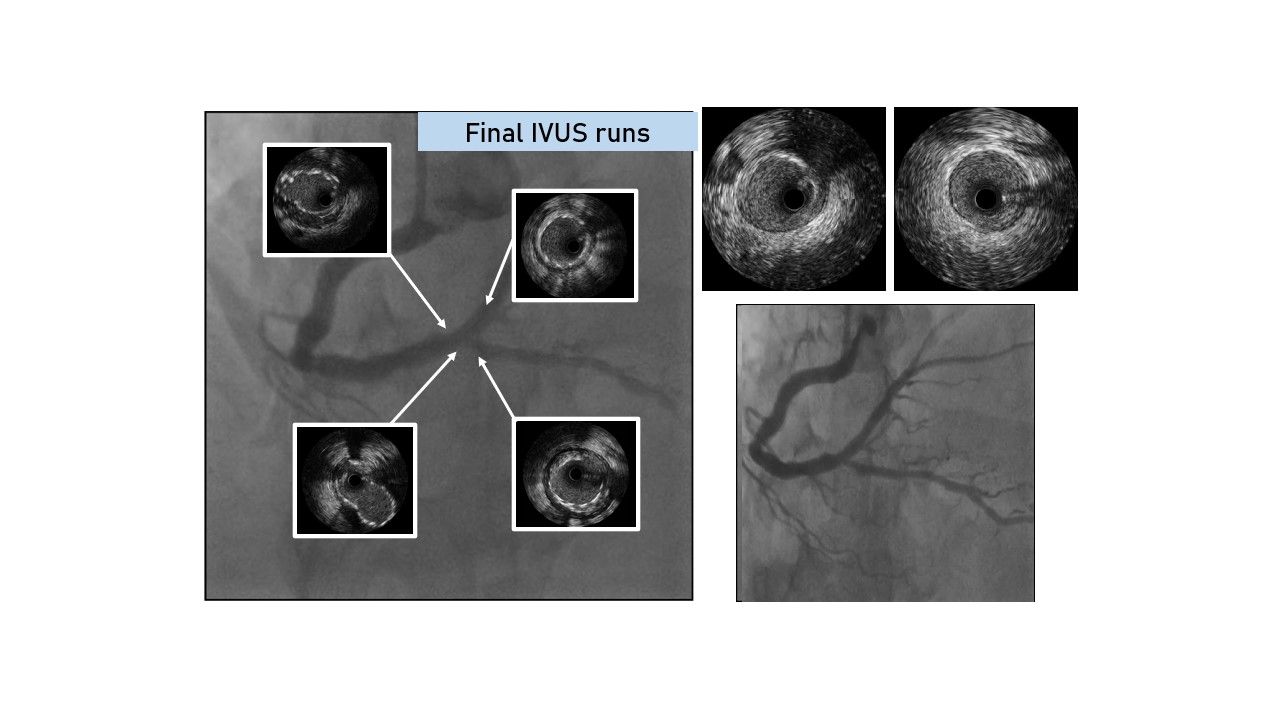
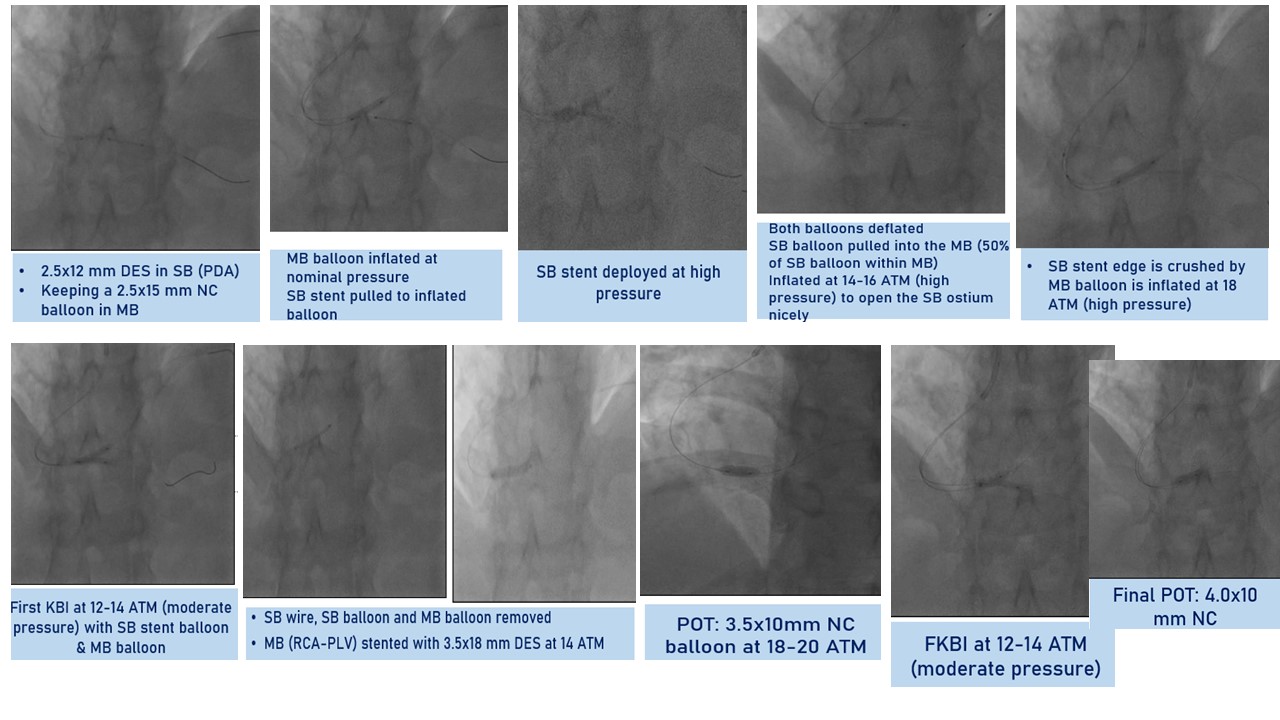
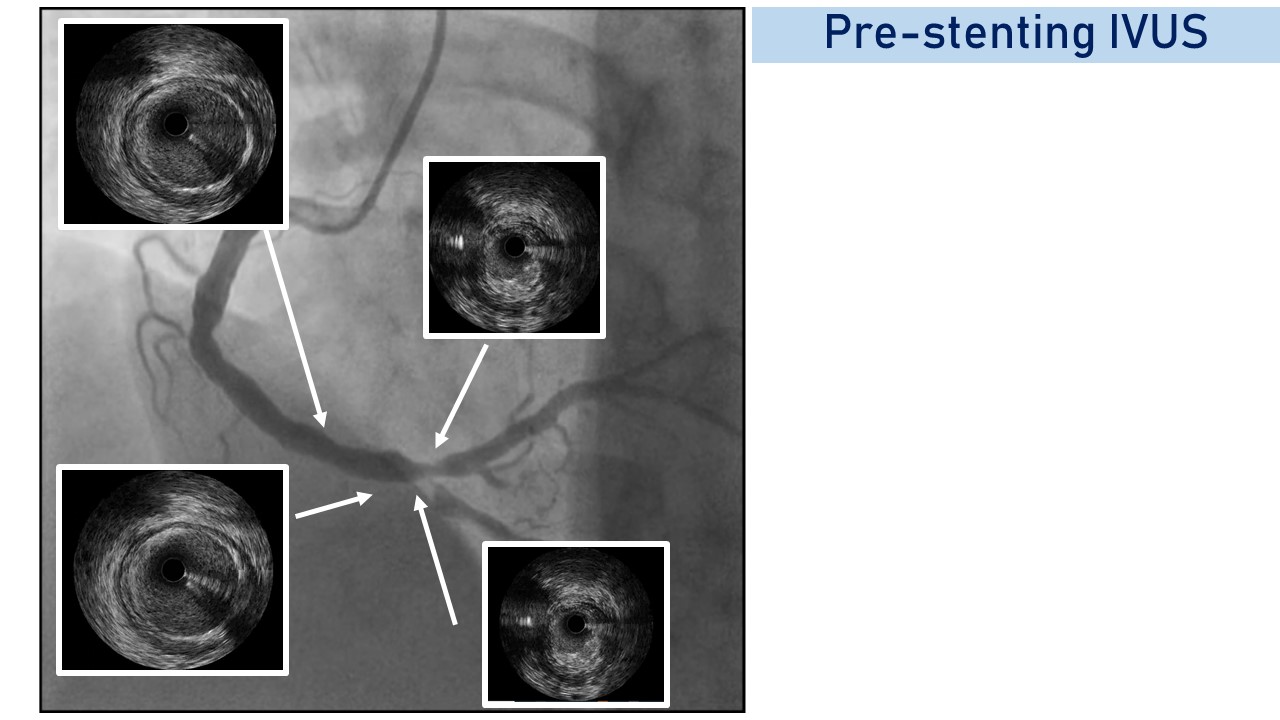
Using a slender approach with JL 3.5 5 Fguide, CTO LAD was crossed with Fielder XT wire and 1.25x5 mm balloon support,confirmed by ipsilateral collaterals. IVUS after predilatation showed focal 270degree calcification with fibrotic plaque and long segment disease. LAD was stented by 2.25x40 mm DES at 12 ATM, keeping the stent just below thebifurcation, not to jail he diagonal branch as IVUS showed no diseaseprogression in LAD at the level of the Diagonal. It was postdilated with good angiographic and IVUSresult. As IVUS showed plaque burden at both the PDA and PLV ostia, we decidedto go two-stent strategy. JR 3.5 6 Fguide was engaged in the RCA. To minimise procedural complexity, nano-crush wasadopted for distal RCA bifurcation. PDA and PLV were wired. PDA was stented by2.5x15mm DES, keeping a 2.5x15 mm NC balloon in main branch (MB), which wasused to crush side branch (SB) stent and kissing balloon inflation (KBI). Bothballoons were deflated. 50% of SBballoon was pulled into the MB and inflated at 14-16 ATM, to open the SB ostium.SB stent edge was crushed. POT was done by 3.5x10mm NC balloon at 18-20 ATM. SBwas rewired through middle strut of the MB. FKBI was done at 12-14 ATM. FinalPOT was done by 4.0x10 mm NC balloon at 16ATM with good angiographic and IVUSresults.
Case Summary
Complete revascularization in case of double jeopardy in STEMI is justifiable in pharmaco-invasive strategy if haemodynamics, contrast and radiation dose permits. Imaging guidance was crucial in decision-making regarding strategies, and adoption of upfront two-stent strategy of least procedural complexity..