
CASE20210817_004
Challenge for PCI at True Left Main Bifurcation with Multiple Stenosis in Left Circumflex
By ,
Presenter
Novita Sitorus
Authors
1, 1
Affiliation
, Indonesia1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Challenge for PCI at True Left Main Bifurcation with Multiple Stenosis in Left Circumflex
1, 1
, Indonesia1
Clinical Information
Patient initials or Identifier Number
Mr. WS
Relevant Clinical History and Physical Exam
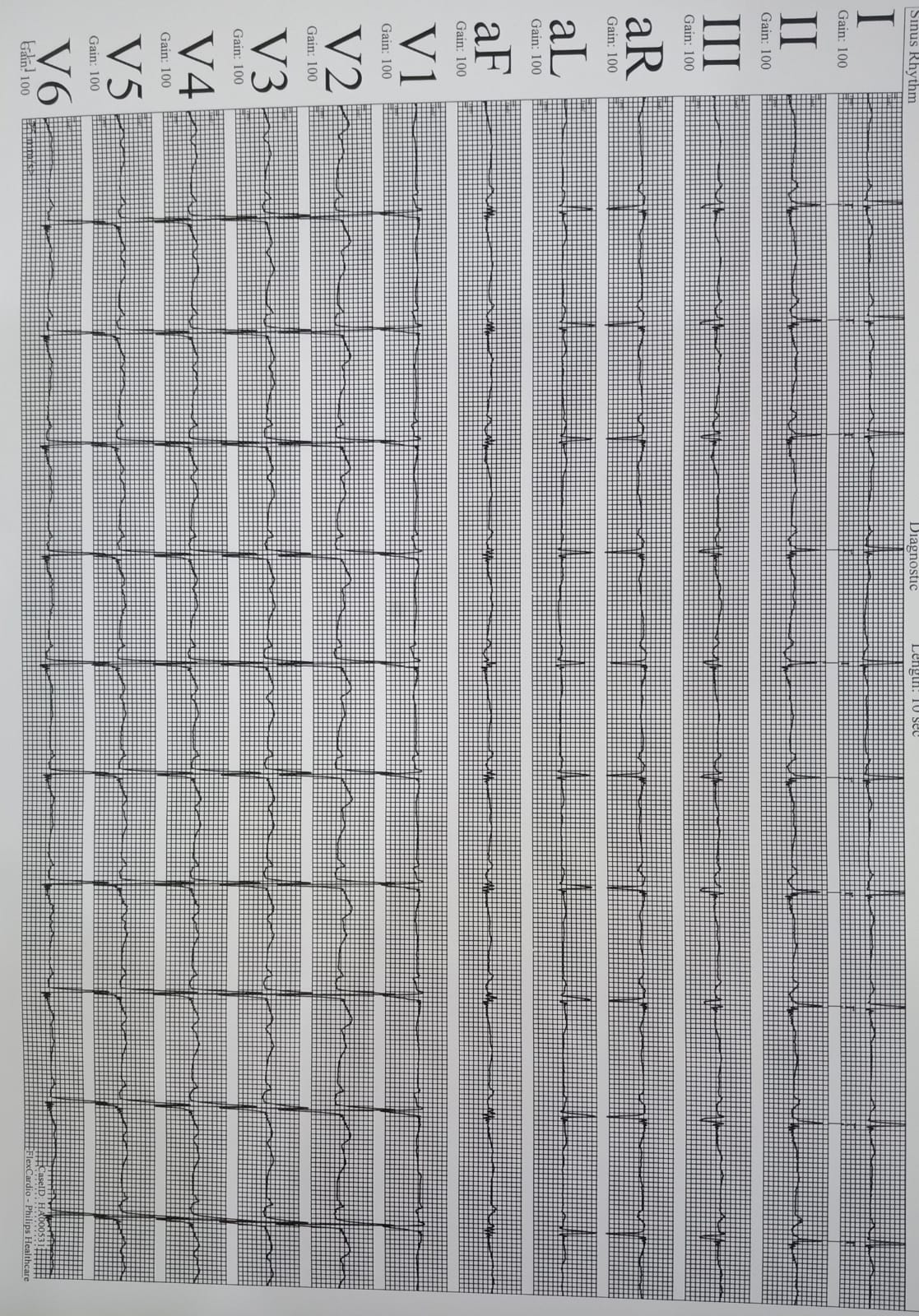
A 61 yo male patient with HT, DM, ex-smokermanifested with APS CCS II. History of PCI with 1 DES at the prox-mid LAD in 2019.Physical examination was normal. Resting ECG showed sinus rhythm withoutabnormal ST-T changes. Echocardiography result was unremarkable(LVEF 56%). The left coronary angiogram showed significant stenosis at distalLM, ostial LAD and ostial LCx (Medina classification 1,1,1). There were multiplesignificant stenosis in LCx and all of branches. Patient refused CABG.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
A 7 Fr sheath through right femoral artery access was inserted. LCA wasengaged with a 3.5/7F XB guiding catheter. A Floppy guide wire (GW) was insertedto LCx. We pre-dilated LCx using scoringballoon 2.5 x10 mm 12 atm at distal, and up to 16 at ostial LCx-LM. Beforestenting distal LCx we put second GW at LAD to protect OM3. A 2.5 x 38 mm DES wasthen inflated up to 13 atm at distal LCx. Considering many OMbranches with significant ostial stenosis that may lost if we do stenting at prox-ostialLCx and potential future PCI to LCx we decided to use DCB to treat thatstenosis. DCB 2.50 x 30 mm up to 17 atm was then inflated for 45” at mid LCx-LM. No dissection nor significant recoilwas seen on evaluation. We proceeded to perform PCI for the LM-LAD. Predilationat LM-LAD was done with 2.5 x 10 mm scoring balloon at 18 atm. A 3.0 x 28 mm DESwas then successfully deployed at prox LAD-LM at17 atm, followed by POT at LM-LAD using NC balloon 4.0 x12 mm,18 atm. GW at LAD was recrossed through distal stent strut at ostial, LCxfollowed by predilated ostial LCx with 2.0 x 10 mm then with NC 2.75x12 mmballoon at 14 atm and finalized with KBT using NC balloon 4.0 x12 mm at LM-LAD up to 10 atm. Final POT at LM-LAD with NC balloon 4.0x12 mmup to 22 atm. No residual stenosis at LM-LAD and 20% at ostial LCx.
 DEB AND DES IN LCX.avi
DEB AND DES IN LCX.avi
FINAL 2020.avi
FINAL CRANIAL.avi
FINAL POT.avi
FINAL SPIDER.avi
FIRST POT.avi
KISS.avi
PRE 2020.avi
PRE SPIDER.avi
STENTING LM LAD.avi
Case Summary
The advent of DCB provides a novel therapeutic strategy for bifurcation lesion by reducing the risk of restenosis due to delivering cytotatic drug thus reducing neointimal hyperplasia. One stent strategycombine with DCB for SB.seem to be a rationale strategy in true LM bifurcation stenosiswhere further PCI to the LCx is potentially needed in the future.