
CASE20210817_003
Rescue PCI of the Bifurcation Lesion with an Aneurysm in the Center after Acute CABG Failure
By ,
Presenter
Sakolwat Montrivade
Authors
1, 1
Affiliation
, Thailand1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Rescue PCI of the Bifurcation Lesion with an Aneurysm in the Center after Acute CABG Failure
1, 1
, Thailand1
Clinical Information
Patient initials or Identifier Number
SL
Relevant Clinical History and Physical Exam
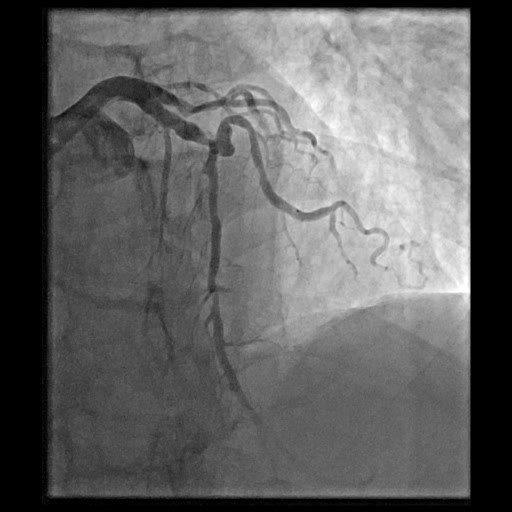
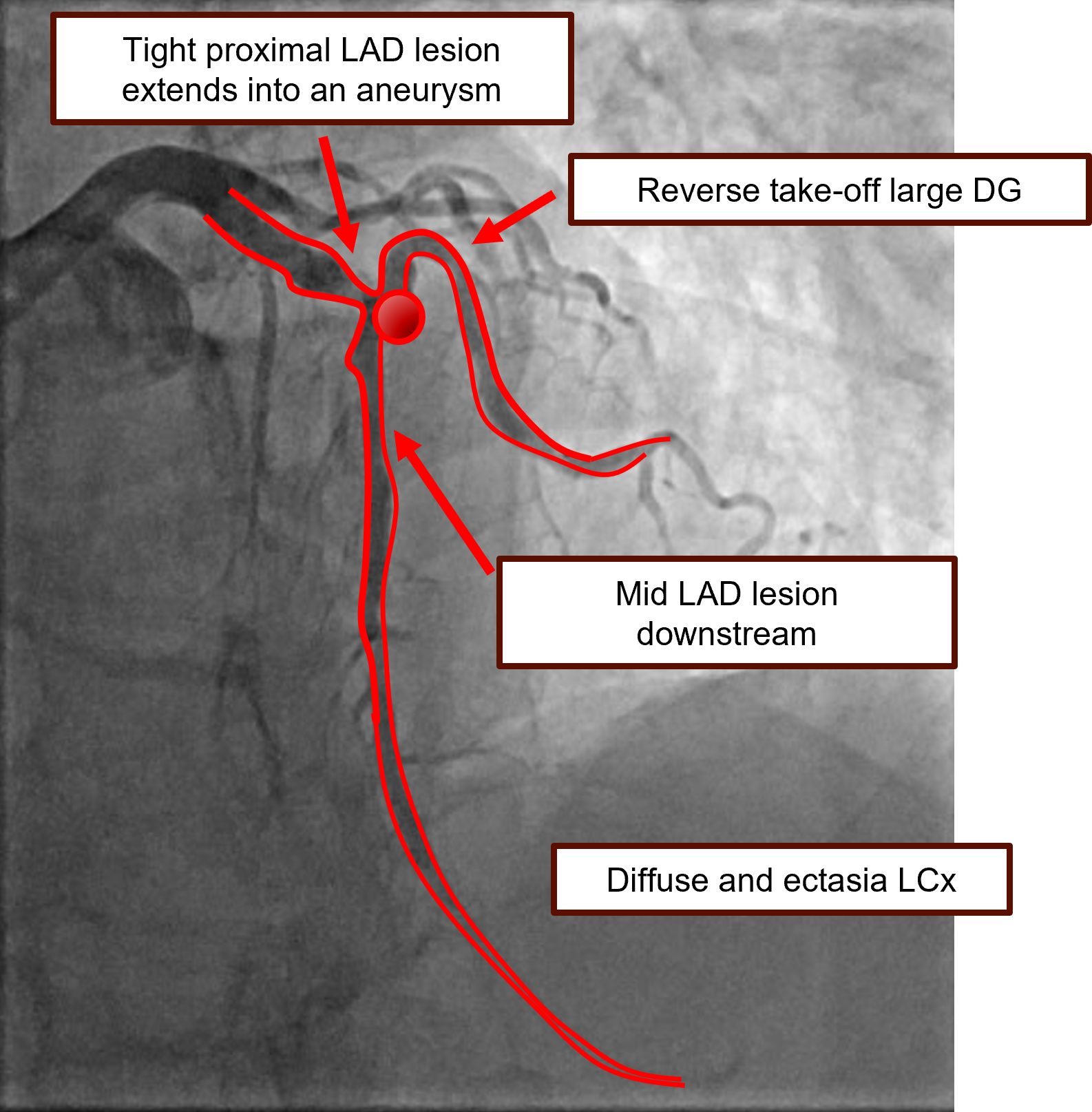
A 62-year-old man presented with an acute anterior wall STEMI for which an emergency CAG revealed a three vessel disease with a significant bifurcation lesion involving a proximal LAD stenosis extending into an aneurysm, mid LAD stenosis and a large DG originating from the aneurysm (Medina 1,1,0). POBA was done and the patient was sent for CABG. LIMA-LAD, SVG-DG and SVG-RCA were grafted. On post-op day 1, the patient had acute heart failure and cardiogenic shock required vasopressors.
Relevant Test Results Prior to Catheterization
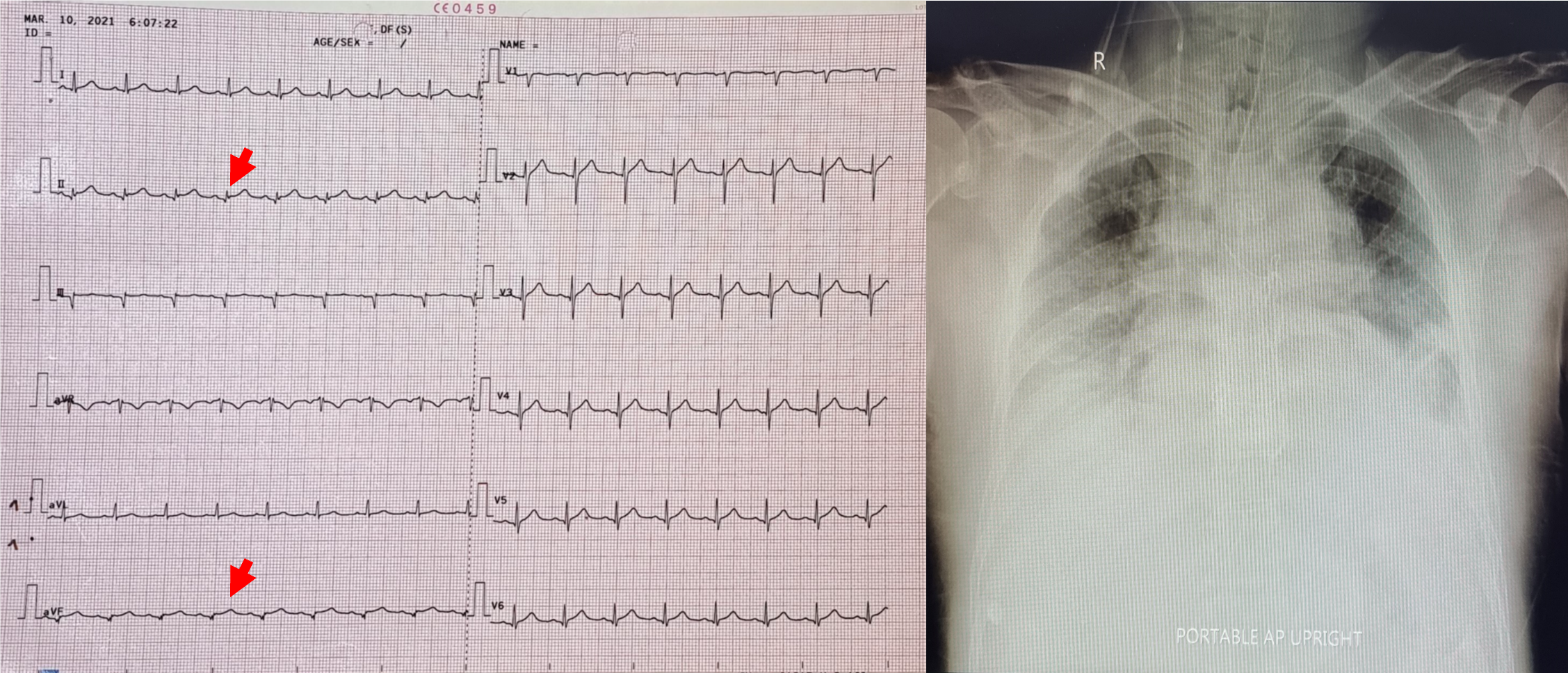
ECG after CABG showed slight ST deviation in lead II and aVF. Chest x-ray revealed pulmonary congestion and endotracheal tube in placed. Cardiac biomarkers obtained after CABG showed rising CK-MB from 48 to 101 ng/mL and elevated hs-troponin T level of 2,330 ng/L.
Relevant Catheterization Findings
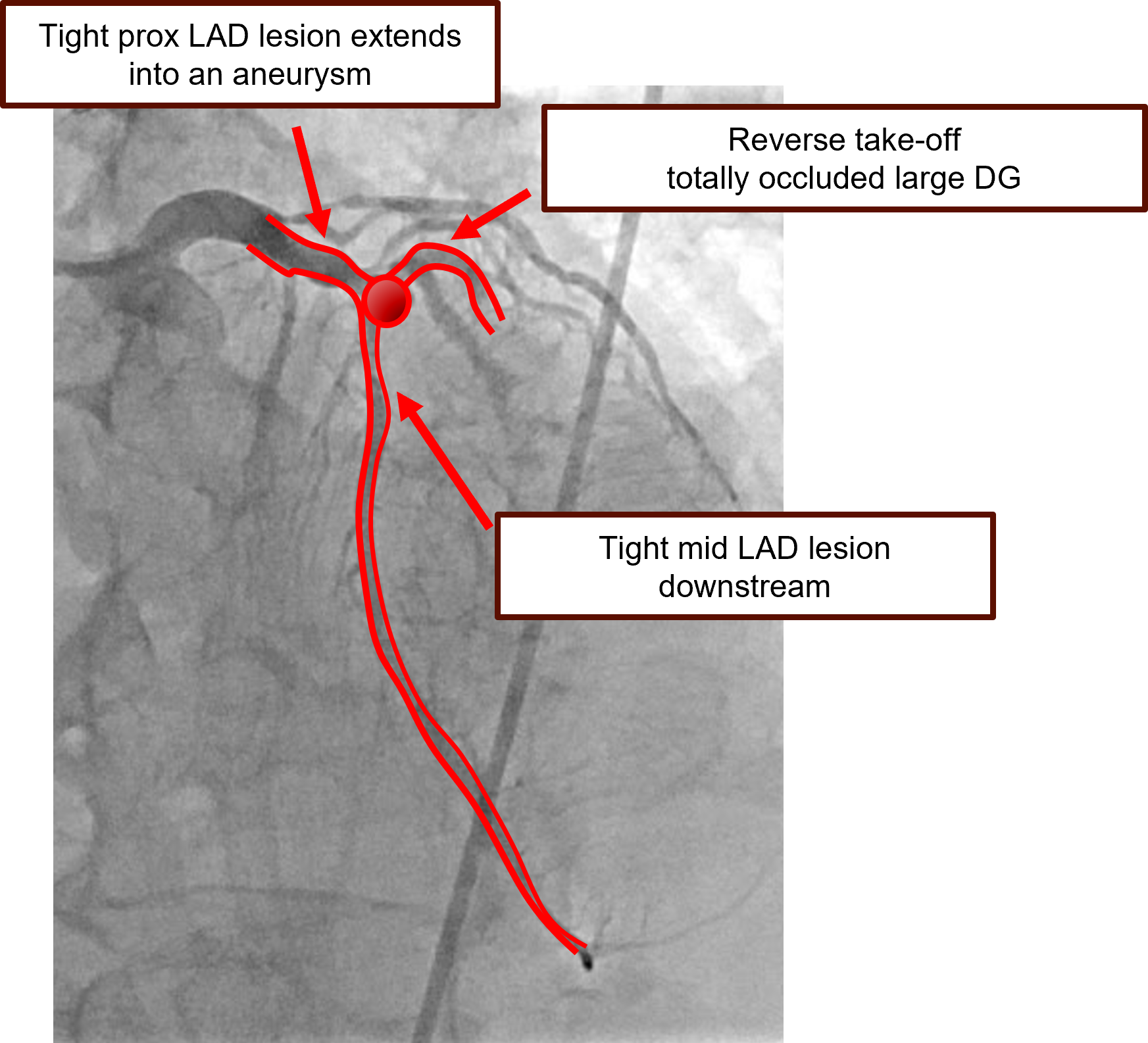
Emergency CAG revealed a right dominant coronary system.LM: no significant stenosis.LAD: 80% stenosis at the proximal LAD extending into an aneurysm, 80% stenosis at the mid LAD and a large DG with 100% total occlusion at the SVG anastomosis.LCx: 90% stenosis at the mid LCx with diffuse ectesia.RCA: 70% stenosis at the distal RCA.LIMA-LAD: 100% occlusion at the body of LIMA graft.SVG-DG: 100% occlusion at the proximal segment of SVG.SVG-RCA: Patent graft.
 01Pre PCI AP cranial.mp4
01Pre PCI AP cranial.mp4
02Fail LIMA.mp4
Interventional Management
Procedural Step
Right femoral access was obtained using 6Fr sheath. IABP was inserted prior to PCI via left femoral artery access. PCI was performed using EBU3.5, 6Fr catheter. Lesion was crossed with Sion Blue wire to distal LAD but DG lesion was unable to cross. Mid LAD was pre-dilated with a 2.5 mm SC balloon at 12 atm and proximal LAD was pre-dilated with a 3.5 mm SC balloon at 12 atm. Mid LAD was stented with a DES (Synergy 2.5 x 20 mm) deployed at 12 atm and proximal LAD was subsequently stented with a DES (Synergy 3.5 x 20 mm) deployed at 12 atm. Both stents were placed precisely just proximal and just distal to the aneurysm leaving a gap between the stents at the aneurysm for DG access. DG lesion was successfully crossed with Fielder XT-R wire in FineCross microcatheter and pre-dilated with a 2.0 mm SC balloon at 6 atm. The DG lesion was stented with a DES (Resolute Onyx 2.25 x 34 mm) placed precisely at the DG ostium. Final angiography revealed TIMI flow III in all three vessels. The 3 stents' edges joined at the aneurysm in the center with minimal protrusion.
03midLAD stent.mp4
04proxLAD stent.mp4
05Final result.mp4
Case Summary
The patient hemodynamics was recovered after PCI and the IABP was removed. After 10 days of hospitalization, the patient was safely discharged.Learning points from this case are as follows:1. There is no optimal approach for PCI of the coronary aneurysm. CABG remains the standard for revascularization of the complex three-vessel disease.2. Acute graft failure is a cause of post CABG complications including HF, ECG changes and hemodynamics collapse.3. PCI of the bifurcation lesion with an aneurysm in the center is challenging. Stenting the lesions with minimal protrusion into the the aneurysm is feasible and safe especially in the emergency and unstable case such as this patient.