
CASE20210810_002
Complications in Cathlab and How to Bail out: Case Series
By
Presenter
Rohit Mody
Authors
1
Affiliation
, India1
Complications - Complications
Complications in Cathlab and How to Bail out: Case Series
1
, India1
Clinical Information
Patient initials or Identifier Number
Case 1- 243941 Case2- 213606 Case3- 107629
Relevant Clinical History and Physical Exam
Case 1-
Patient Details-
56 year old male
Chest Pain
Acute Posterolateral STEMI
Case 2-
Patient Details-
77 year old male
AOE 3
Hypertensive
Diabetic
Dyslipidemic
Case 3-
Patient Details-
54 year old female
AOE 3
Diabetic
Hypertensive
Dyslipidemia
Relevant Test Results Prior to Catheterization
Case 1-Troponin PositiveLV Dysfunction, EF 30%RWMA in Posterolateral RegionECG shows STEMI
Case 2-EF 30%, Global Hypokinesia
Case 3- LV Dysfunction, EF 40%ECG shows Q waves in 2,3 AVF
Case 2-EF 30%, Global Hypokinesia
Case 3- LV Dysfunction, EF 40%ECG shows Q waves in 2,3 AVF
Relevant Catheterization Findings
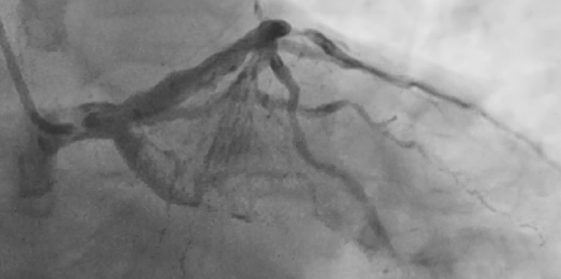
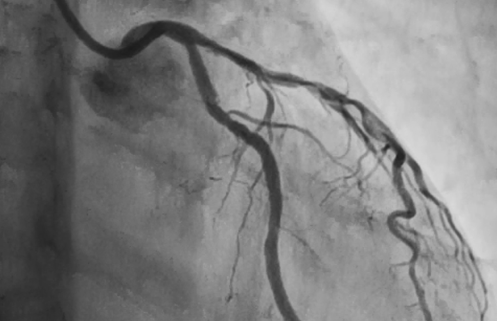
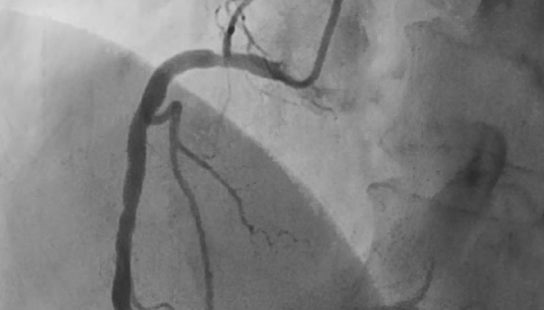
Case 1-Angiography shows TVD planned Culprit vessel PCI to Dominant LCXCase 2- Angiography shows SVD LAD heavily calcifiedCase 3- Angiography shows DVD, The lesion in RCA was borderline
Interventional Management
Procedural Step
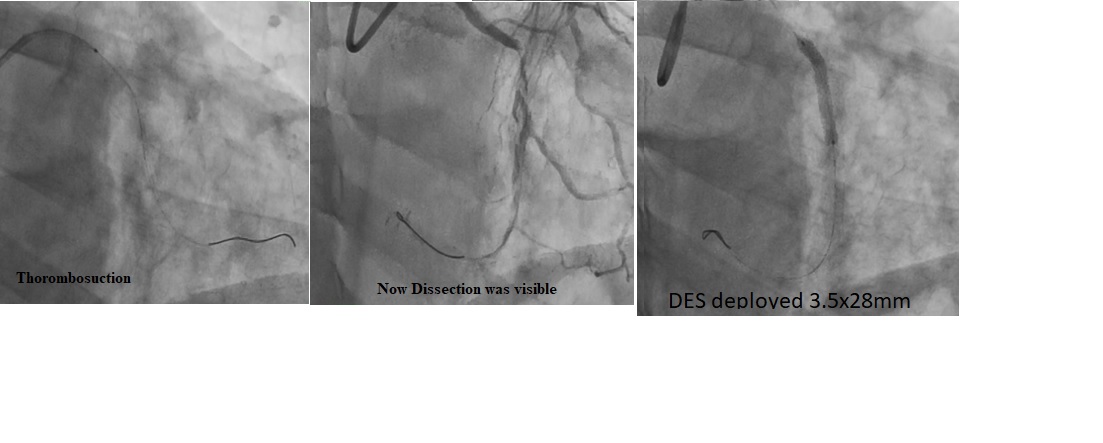
Case1- Tried to cross with Floppy couldn’t cross, There was a knuckle formation & dissection, with great effort crossed with Floppy wire through dissection,Balloon dilated with 1.5mm balloon, Thrombosuction, Pre-Dilatation with 2.5mm balloon, Now Dissection was visible , DES deployed 3.5x28mm at 10ATM,
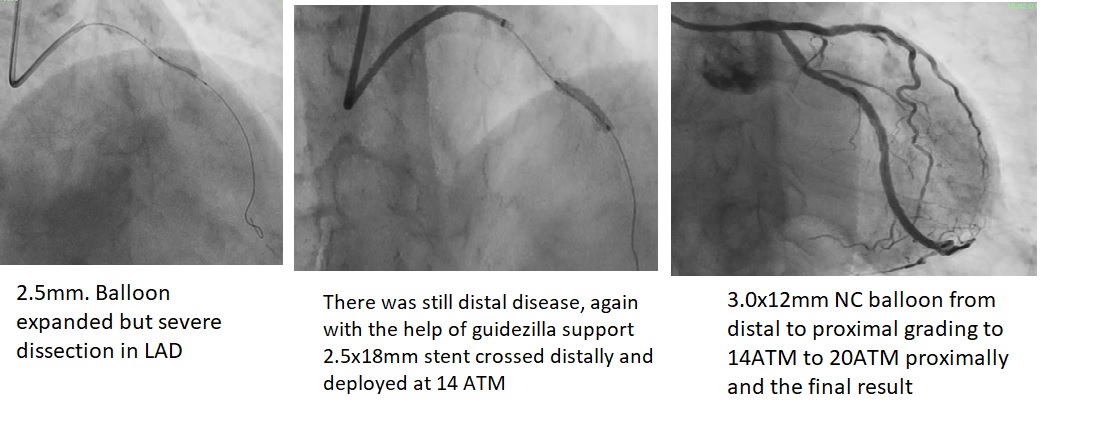
Case2- Balloon dilated with 2.5mm. Balloon expanded but severe dissection in LAD, 2.5x30mm stent and 2.5x18mm stent unable to cross the lesion. The Buddy wire technique with two wires failed, There was a calcified Spur, the first stent 2.5x18mm was unable to cross distally, guidezilla support from LAD taken & Stent Deployed, There was still distal disease, again with the help of guidezilla support 2.5x18mm stent crossed distally and deployed at 14 ATM, Finally post dilated with 3.0x12mm NC balloon from distal to proximal grading to 14ATM to 20ATM proximally and the final result.
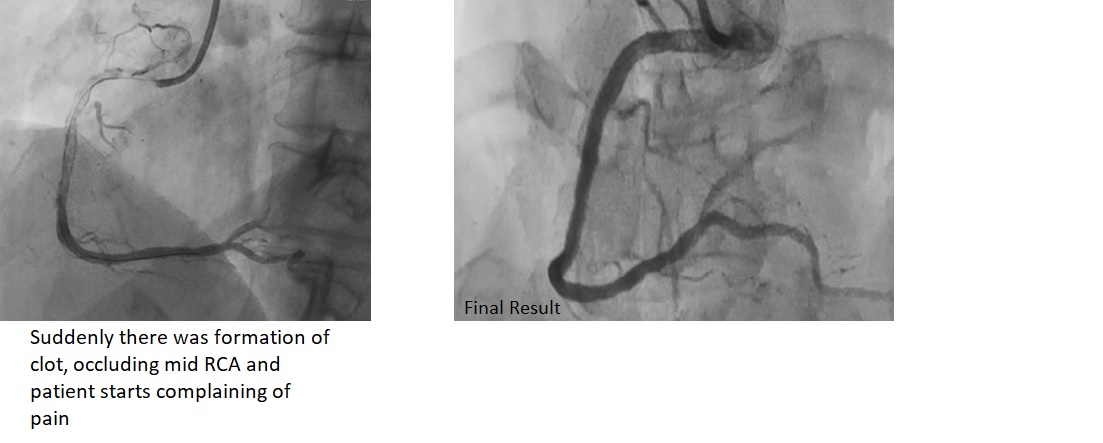
Case3- Crossed with wire, And IVUS run was taken the disease in RCA had plaque burden was around 65% hence decided to stent, Suddenly there was formation of clot, occluding mid RCA and patient starts complaining of pain, Direct stent placed across the clot and stent deployed at 12 ATM compressing the stent,
Case2- Balloon dilated with 2.5mm. Balloon expanded but severe dissection in LAD, 2.5x30mm stent and 2.5x18mm stent unable to cross the lesion. The Buddy wire technique with two wires failed, There was a calcified Spur, the first stent 2.5x18mm was unable to cross distally, guidezilla support from LAD taken & Stent Deployed, There was still distal disease, again with the help of guidezilla support 2.5x18mm stent crossed distally and deployed at 14 ATM, Finally post dilated with 3.0x12mm NC balloon from distal to proximal grading to 14ATM to 20ATM proximally and the final result.
Case3- Crossed with wire, And IVUS run was taken the disease in RCA had plaque burden was around 65% hence decided to stent, Suddenly there was formation of clot, occluding mid RCA and patient starts complaining of pain, Direct stent placed across the clot and stent deployed at 12 ATM compressing the stent,
Case Summary
In crossing 100% soft occlusion can cause dissection which can be negotiated with CTO skills.
• In calcified lesions sometimes stent doesn’t cross even buddy wire fails use of guideliner is handy in such situations.
• Sometimes suddenly you see abundant clot from catheter into coronary artery most likely due to reduced ACT can be bailed out by direct stenting.