
CASE20210730_001
Ticagrelor-Associated High-Degree Heart Block: A Case Report & Review of the Literature
By
Presenter
Hariom Tyagi
Authors
1
Affiliation
, India1
High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention
Ticagrelor-Associated High-Degree Heart Block: A Case Report & Review of the Literature
1
, India1
Clinical Information
Patient initials or Identifier Number
a
Relevant Clinical History and Physical Exam
T2DM/CAD/ACS/RECENT IWMI/POST CAG-TVD/POST PTCA TO LCXTO OM (02.12.2018)/MILD LV SYSTOLIC DYSFUNCTION/LVEF=40-45%/MILD MR/PTCA TO RCA& RAMUS (10.01.2019) AV NODE DYSFUNCTION (ON TPI)/PPI- MICRA-MCIVR01 in RV
Relevant Test Results Prior to Catheterization
Left Main: Normal.
Relevant Catheterization Findings
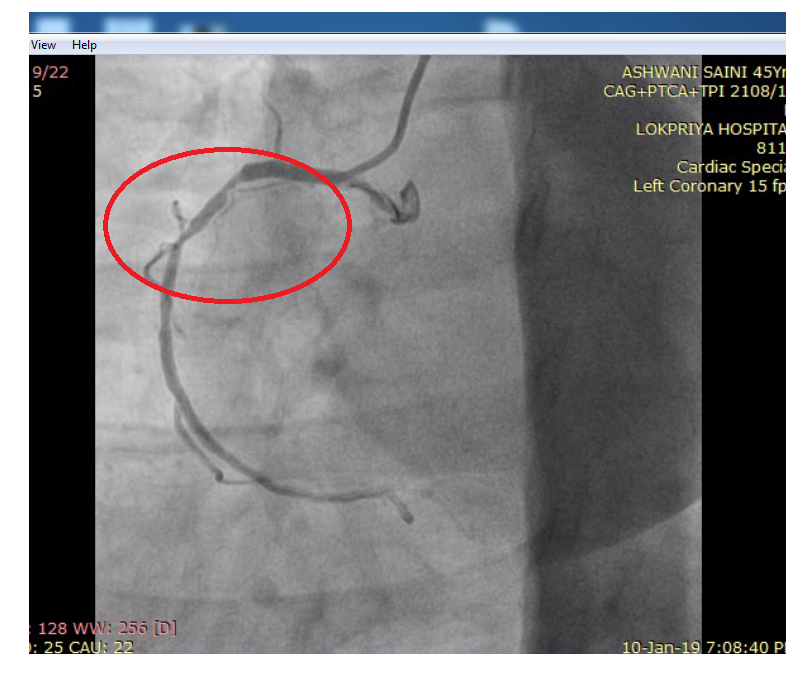
PTCA TO RCA: Right Coronary Artery was engaged with JR 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the RCA lesion. Direct stenting was done with Drug Eluting Stent PROMUS ELEMENT 3.5 × 38 mm was deployed in RCA @ 12 atmosphere. Post dilatation done with NC sapphire balloon 3.5 × 10 mm @ 20 atmosphere.PTCA TO RAMUS: In same sitting, Left Coronary Artery was engaged with EBU 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the RAMUS lesion. Direct sten.

Interventional Management
Procedural Step
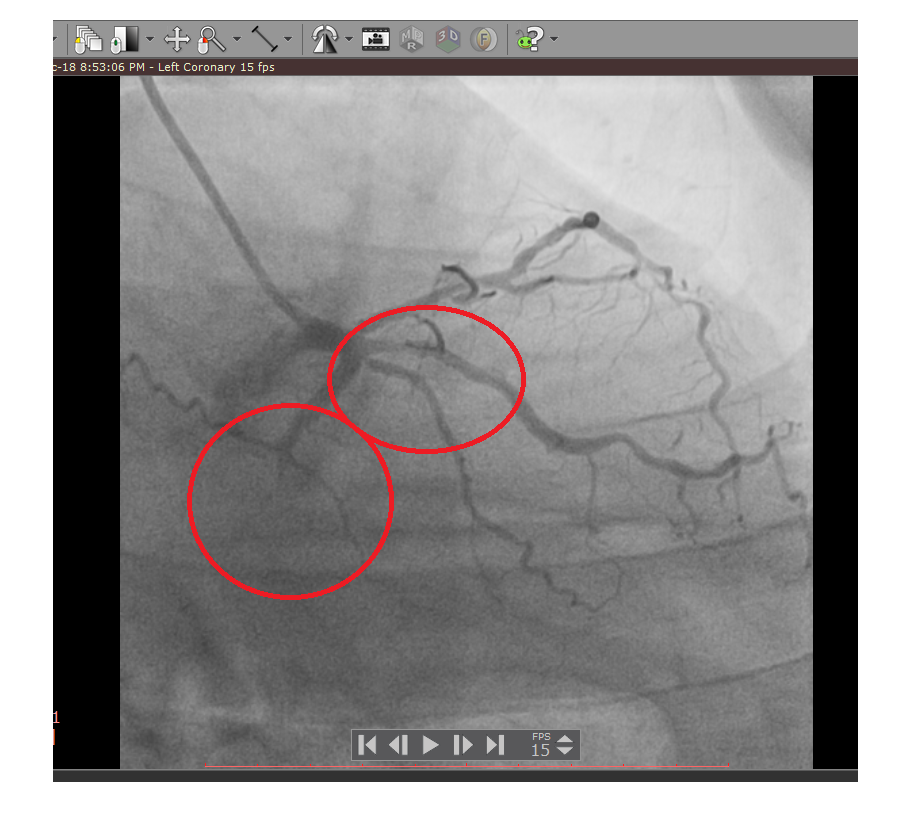
Left Coronary Artery was engaged with EBU 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the LCX & OM lesion. Pre dilatation done with SC sapphire balloon 2.0 × 10 mm @ 16 atmosphere. Drug Eluting Stent RESOLUTE ONYX 2.75 × 18 mm was deployed in LCX @ 16 atmosphere & another Drug Eluting Stent PROMUS ELEMENT 2.5 × 24 mm was deployed in OM @ 16 atmosphere. Post dilatation done with NC sapphire balloon 3.5 × 10 mm @ 18 atmosphere. GP IIb IIIa inhibitor was used during the procedure. Excellent result with TIMI III flow. PTCA TO RCA: Right Coronary Artery was engaged with JR 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the RCA lesion. Direct stenting was done with Drug Eluting Stent PROMUS ELEMENT 3.5 × 38 mm was deployed in RCA @ 12 atmosphere. Post dilatation done with NC sapphire balloon 3.5 × 10 mm @ 20 atmosphere. PTCA TO RAMUS: In same sitting, Left Coronary Artery was engaged with EBU 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the RAMUS lesion. Direct stenting was done with Drug Eluting Stent RESOLUTE ONYX 2.75 × 22 mm was deployed in RAMUS @ 12 atmosphere. Post dilatation done with NC sapphire balloon 3.5 × 10 mm @ 12 atmosphere.
 TICAGRELOR ASSOCIATED HIGH DEGREE HEART BLOCK A CASE REPORT REVIEW OF THE LITERATURE1.pptx
TICAGRELOR ASSOCIATED HIGH DEGREE HEART BLOCK A CASE REPORT REVIEW OF THE LITERATURE1.pptx
Case Summary
We present a case of symptomatic and profound AV node dysfunction in a patient treated with ticagrelor post-PCI for Inferior Wall MI. This was observed in our patient even in the absence of baseline conduction disease or concurrent confounding medications, unlike most cases in the published literature and highlights the need for broader awareness of ticagrelor’s not-insignificant brady-arrhythmic potential.