
CASE20210727_002
Ostial Disease, Spontaneous Dissection: The Perfect Bifurcation Technique, Proven by IVUS
By
Presenter
Mario Bollati
Authors
1
Affiliation
, Italy1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Ostial Disease, Spontaneous Dissection: The Perfect Bifurcation Technique, Proven by IVUS
1
, Italy1
Clinical Information
Patient initials or Identifier Number
MM
Relevant Clinical History and Physical Exam
A 40 years old lady came to our hospital for chest pain at rest, unstable, since one day.Cardiovascular risk factors: active smoker
Previous general hisotry: not significant
Previous cardiovascular history: negative
Previous general hisotry: not significant
Previous cardiovascular history: negative
Relevant Test Results Prior to Catheterization
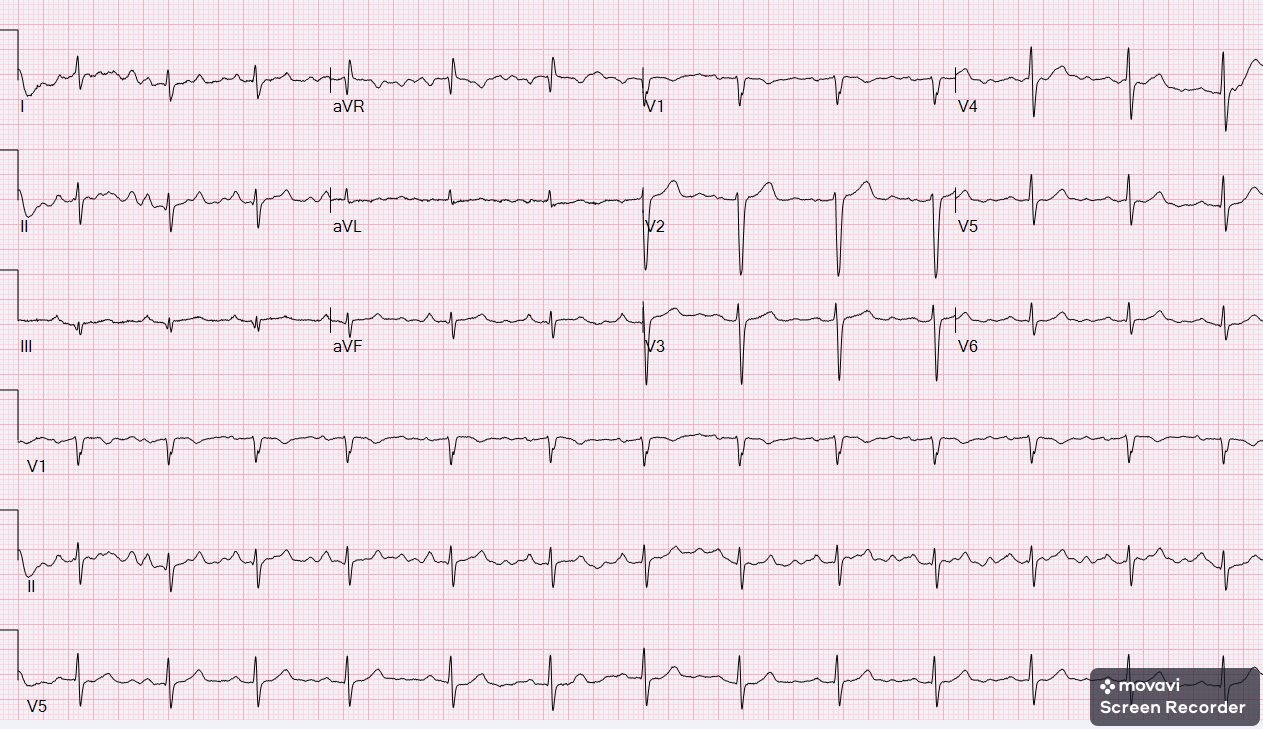
The EKG was nearly normal, echocardiogram showed mid portion inferior wall hypokinesia. Troponine was 12.000 ng/L (normal level under 12 ng/L). Due the NSTEMI diagnosis, the lady was scheduled for urgent coronary angiogram.
Relevant Catheterization Findings
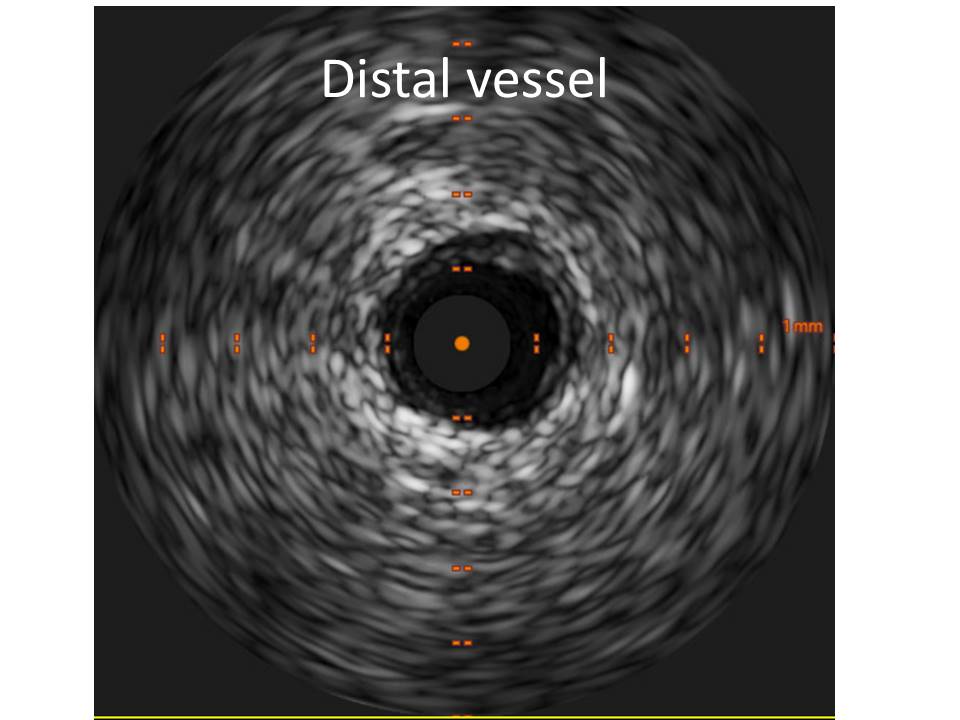
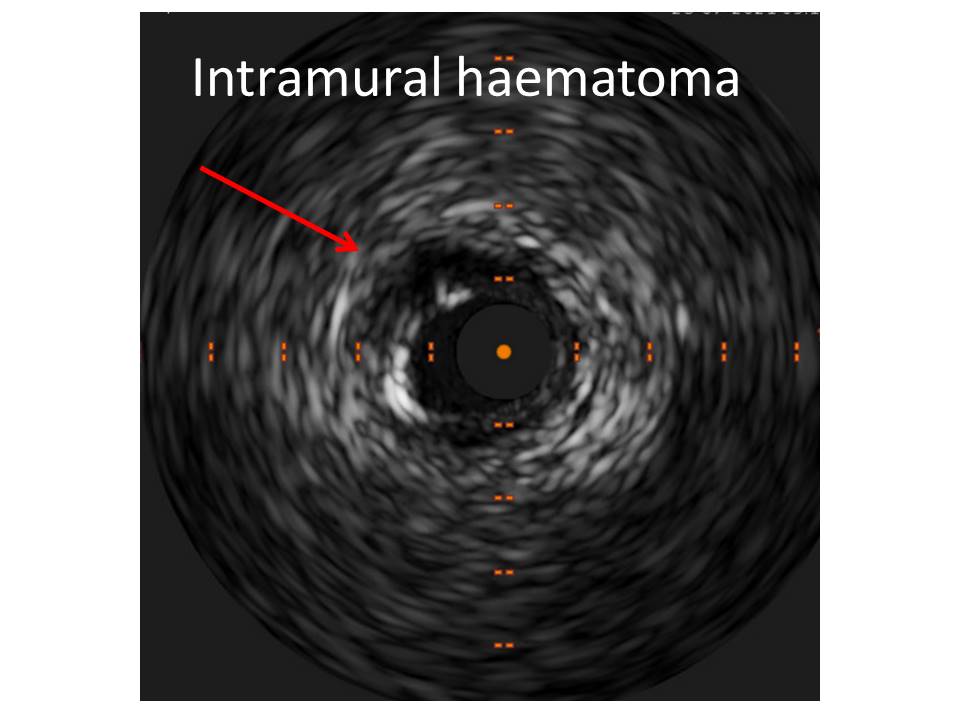
Corknaroy angiography showed an ostial right coronary artery spontaneous dissection, with distal TIMI III flow.IVUS imaging showe subendothelial haematoma with minimal luminal area reduction at proximal-ostial part.
 ScreenRecorderProject5.mp4
ScreenRecorderProject5.mp4
Interventional Management
Procedural Step
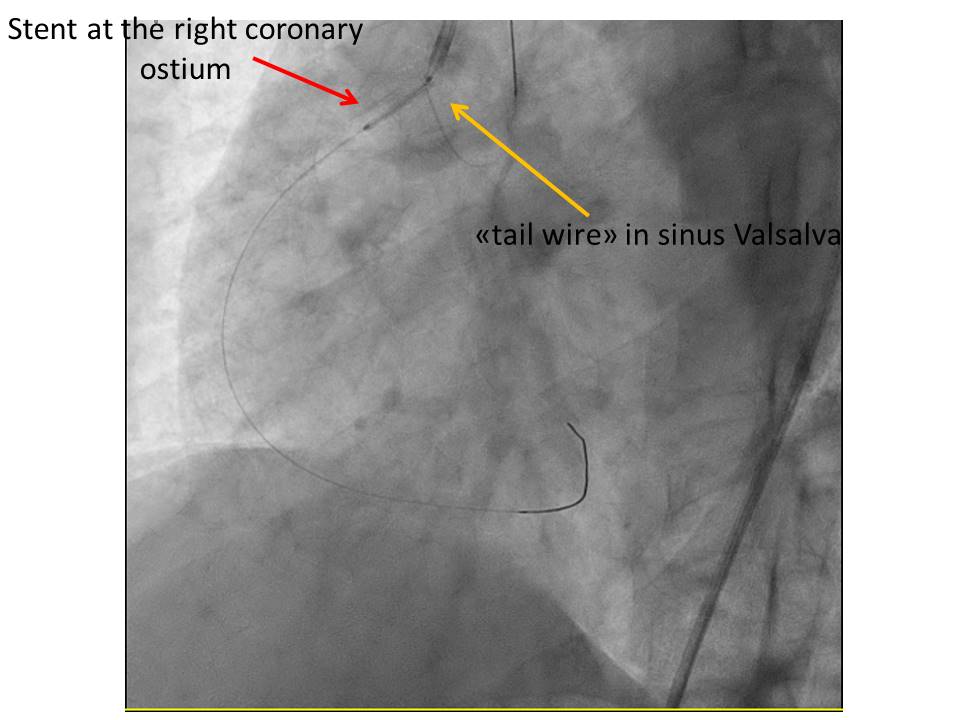
PCI with Xience 3.0/23 (Abbott Laboratories, Illinois, USA) was done in proximal right.Due catheter instability, considering the full ostium coverage as a key point to seal the dissection, a second stent (Xience 3.0/15) has been implanted at ostium level using the "Szabo technique", also kown as "tail wire technique". In this technique, a "stop wire" is placed across the last strut of the stent, facilitating the proximal stent placing just at the ostium, reducing strut protusion and allowing a good full coverage.The steps are:1- Outside of the catheter, the stent cover is removed partially, uncovering the proximal strut.2- The stent is inflated at 2-4 atm, in order to partially open the proximal stent strut.3- The distal part of a second coronary wire (placed in aorta) crosses the opened strut.4- The stent is advanced up the aorto-ostial lesion: the second wire stops the stent just at the ositum (given the resistance against the aortic wall).5- The stent is normally implanted and the second wire is removed.6- Final flair is done as usual.
ScreenRecorderProject1.mp4
ScreenRecorderProject8.mp4
Case Summary
Aorto ostial lesion and bifurcation in general represent a challenging condition for PCI, due the difficult to ensure full ostium coverage, minimal stent protusion in the main vessel/aorta, complete apposition.Szabo technique allows to obtain very good results, acquiring complete ostium coverage with minimal protrusion and malapposition. Anyway, bifurcation is a three-dimensional entity, and "tail wire" technique is not a good result warranty. In this contest, IVUS imaging may be useful to determine the real threedimesional anatomy ot the vessel.