
CASE20210724_001
Double Culprit STEMI
By ,
Presenter
Chun Lin Raymond Cheung
Authors
1, 1
Affiliation
, Hong Kong, China1
High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention
Double Culprit STEMI
1, 1
, Hong Kong, China1
Clinical Information
Patient initials or Identifier Number
Mr Tang
Relevant Clinical History and Physical Exam
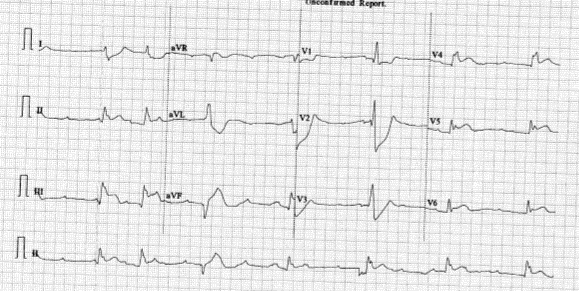
Mr Tang, a 61 year old man, was admitted to our hospital on 12/6 for chest pain since 1am, associated with sweating, dizziness and vomiting.
Relevant Test Results Prior to Catheterization
Bedside vscan
Relevant Catheterization Findings
Coro results:
Conclusion double culprit STEMI, planning for primary PCI to LAD and RCA.
RCA was engaged with JR 3.5 6F.
LM was engaged with JL3.5 6Fr.
Successful PCI to LAD and RCA done.
 leftcoro2.avi
leftcoro2.avi
leftcoro1.avi
rightcoro.avi
Conclusion double culprit STEMI, planning for primary PCI to LAD and RCA.
RCA was engaged with JR 3.5 6F.
LM was engaged with JL3.5 6Fr.
Successful PCI to LAD and RCA done.
Interventional Management
Procedural Step
But patient remained in severe shock, SBP ~ 40despite succssful PCI.
Staged PCI done on 16/6/2021.
IVUS showed RCA distal stent landed on plaque.
IVUS showed LAD stent mild malapposition and underexpansion.
ECMO was removed before the patient left the catherization lab.Impella was removed on day 8.
Serial Echo showed improving LV and RV function.
leftpci1.avi
leftpci2.avi
rightpci.avi
Staged PCI done on 16/6/2021.
IVUS showed RCA distal stent landed on plaque.
IVUS showed LAD stent mild malapposition and underexpansion.
ECMO was removed before the patient left the catherization lab.Impella was removed on day 8.
Serial Echo showed improving LV and RV function.
Case Summary
This case illustrated with a difficult scenario where a patient had both cardiogenic shock and STEMI at the same time. It is difficult to decide to deal with which problem first in order to stabilize the patient. It depends on a number of factors, including vitals, difficulty in stenting, availability or time to set up mechanical circulatory support. Each case is different and difficult. It requires experience, careful consideration and perhaps some luck to save patients successfully.