
CASE20210716_002
The Crusade Microcatheter-Facillated Technique in Complex and Long Chronic Total Occlusion Case
By ,
Presenter
Meng-Ying Lu
Authors
1, 1
Affiliation
, Taiwan1
Complex PCI - Chronic Total Occlusion
The Crusade Microcatheter-Facillated Technique in Complex and Long Chronic Total Occlusion Case
1, 1
, Taiwan1
Clinical Information
Patient initials or Identifier Number
WG,T
Relevant Clinical History and Physical Exam
A 68-year-old gentleman with hypertension, and heart failure with reduced ejection refraction, complained of effort angina when he was going upstairs for one month.
He denied paroxysmal nocturnal dyspnea or orthopnea. Physical examination revealed regular heart beat, no cardiac murmur, no S3/S4, clear breathing sound, and bilateral leg pitting edema, Grade 1.
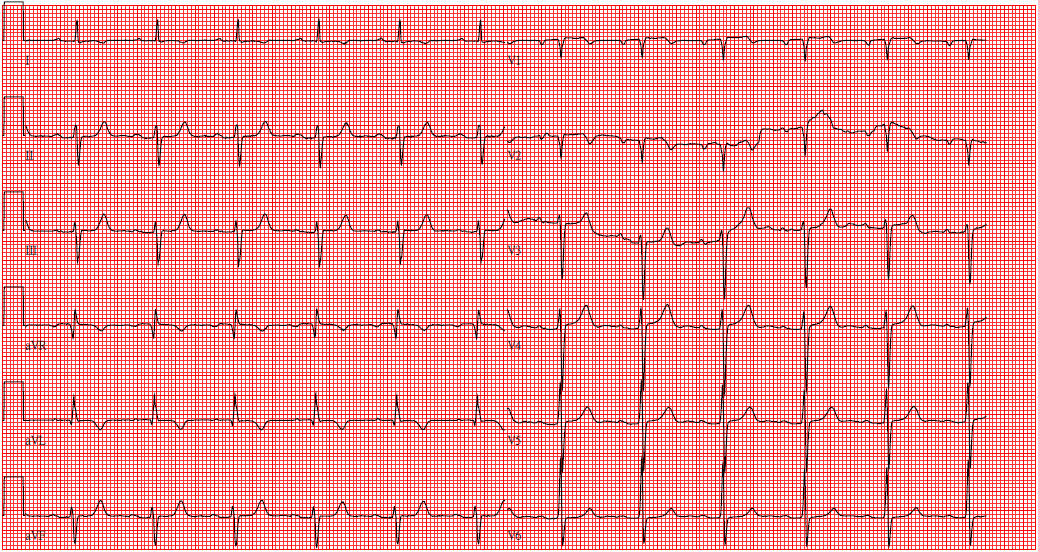
Relevant Test Results Prior to Catheterization
1. Heart echo: Impaired LV systolic and diastolic function with LVEF = 48 % 2. Myocardial perfusion scan:The scintigraphic findings suggest severe ischemia, mostly in the LAD territory.
Relevant Catheterization Findings
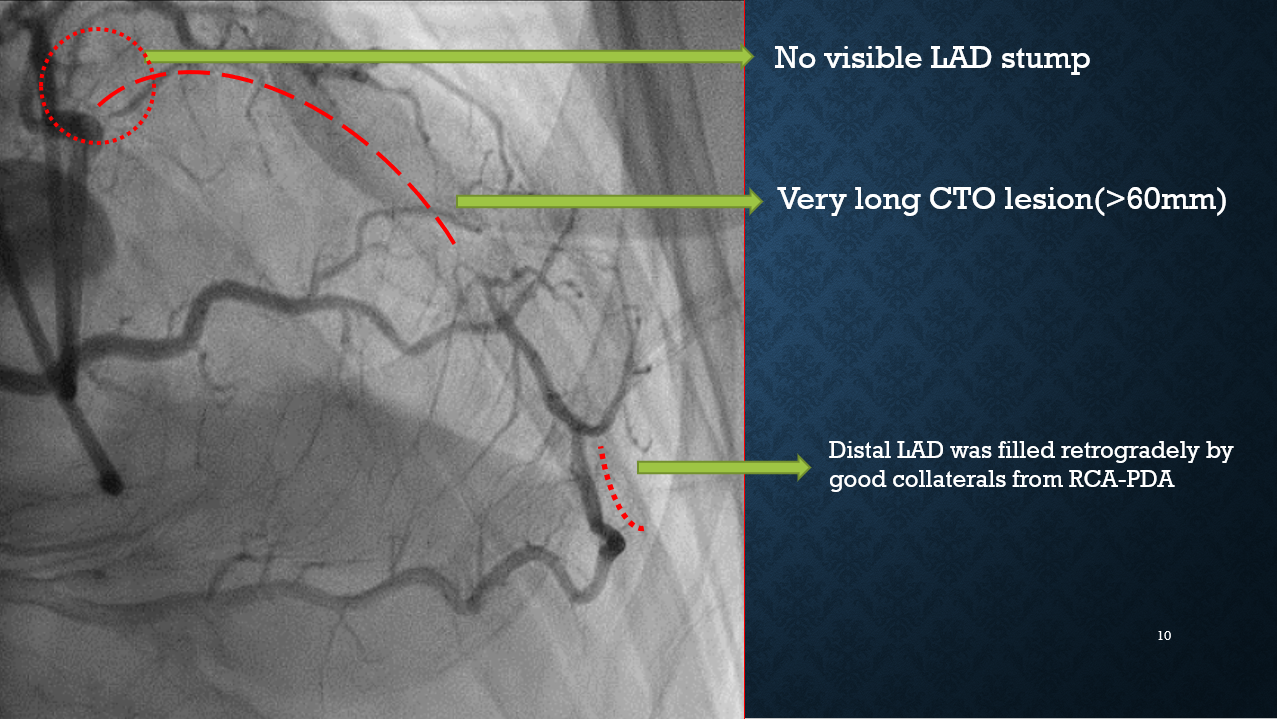
CAG findings: CAD with SVD
1. LAD ostium CTO, with Collateral arteries from RCA-PDA, RCA-PLV to LAD-m and LAD-d
2. J-CTO score = 3, CTO length > 60 mm
3. No visible LAD stump
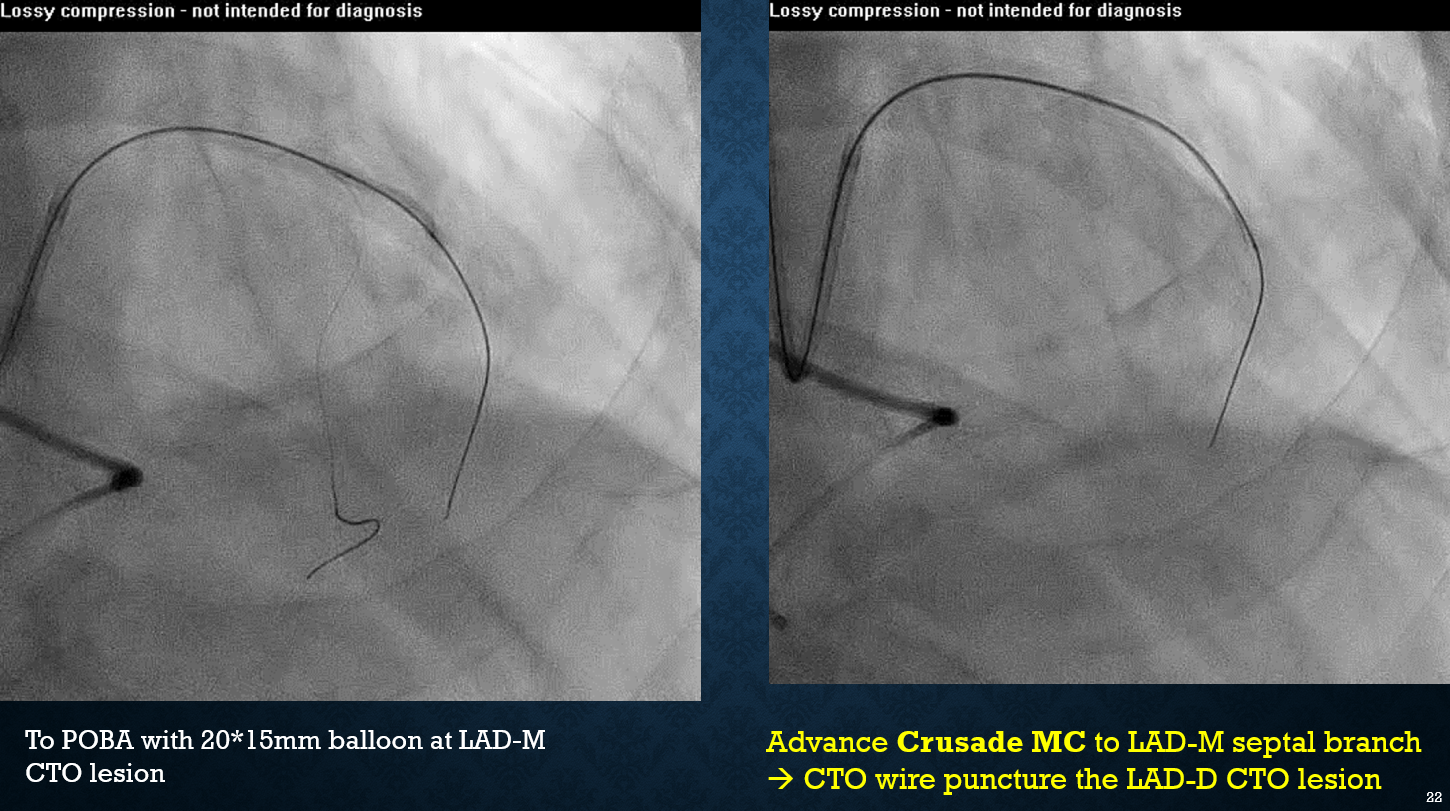
Interventional Management
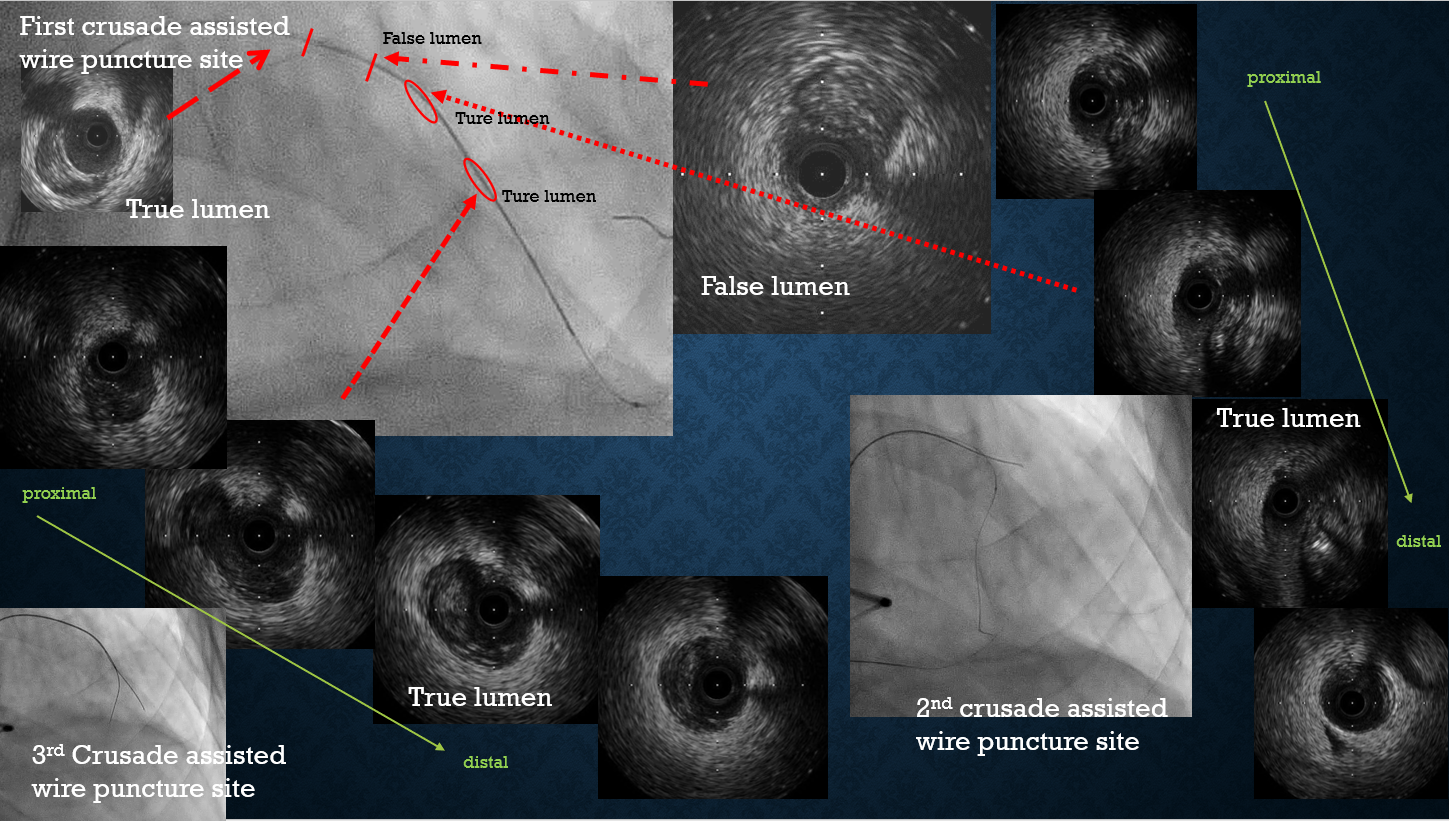
Procedural Step
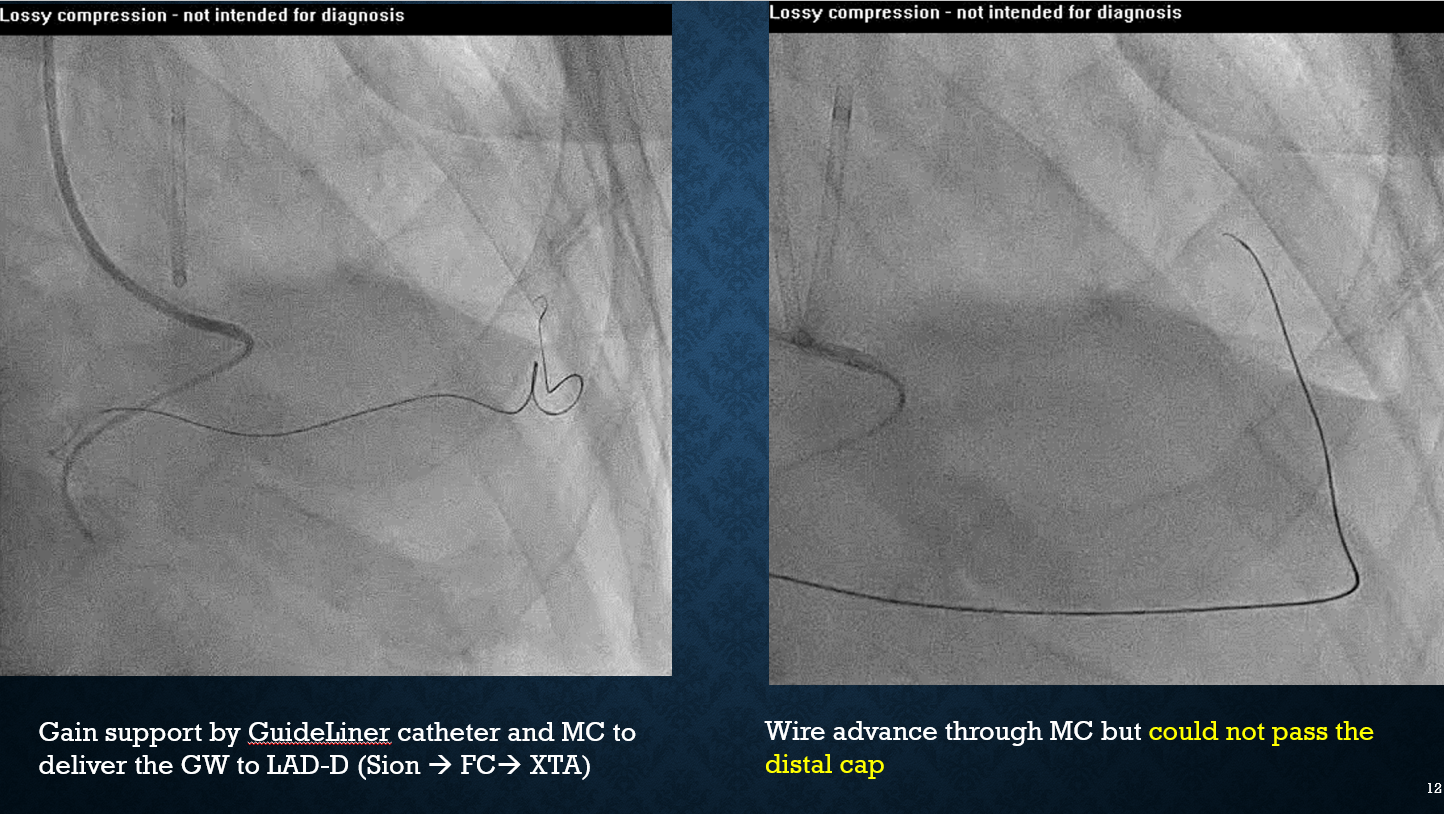
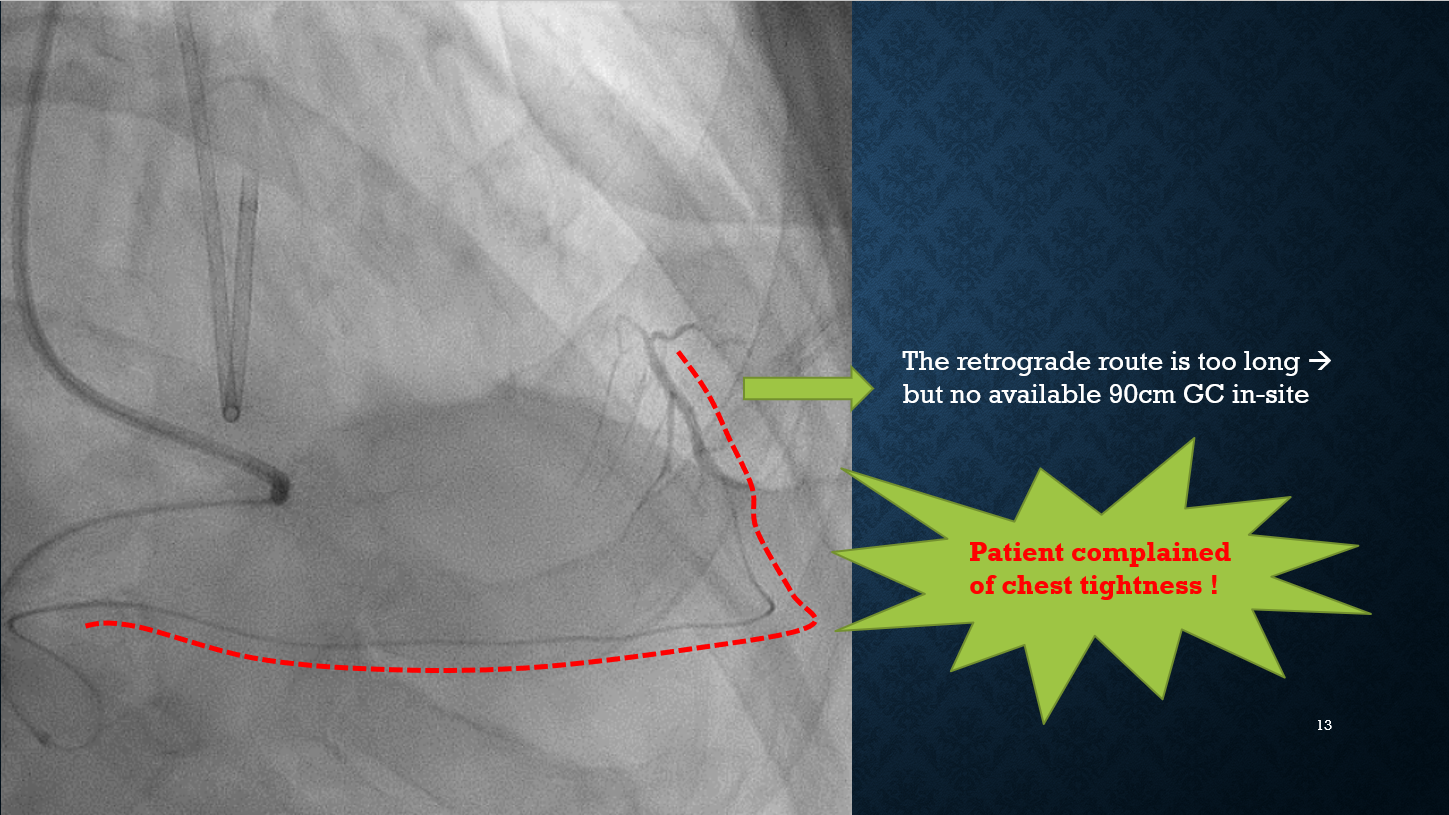
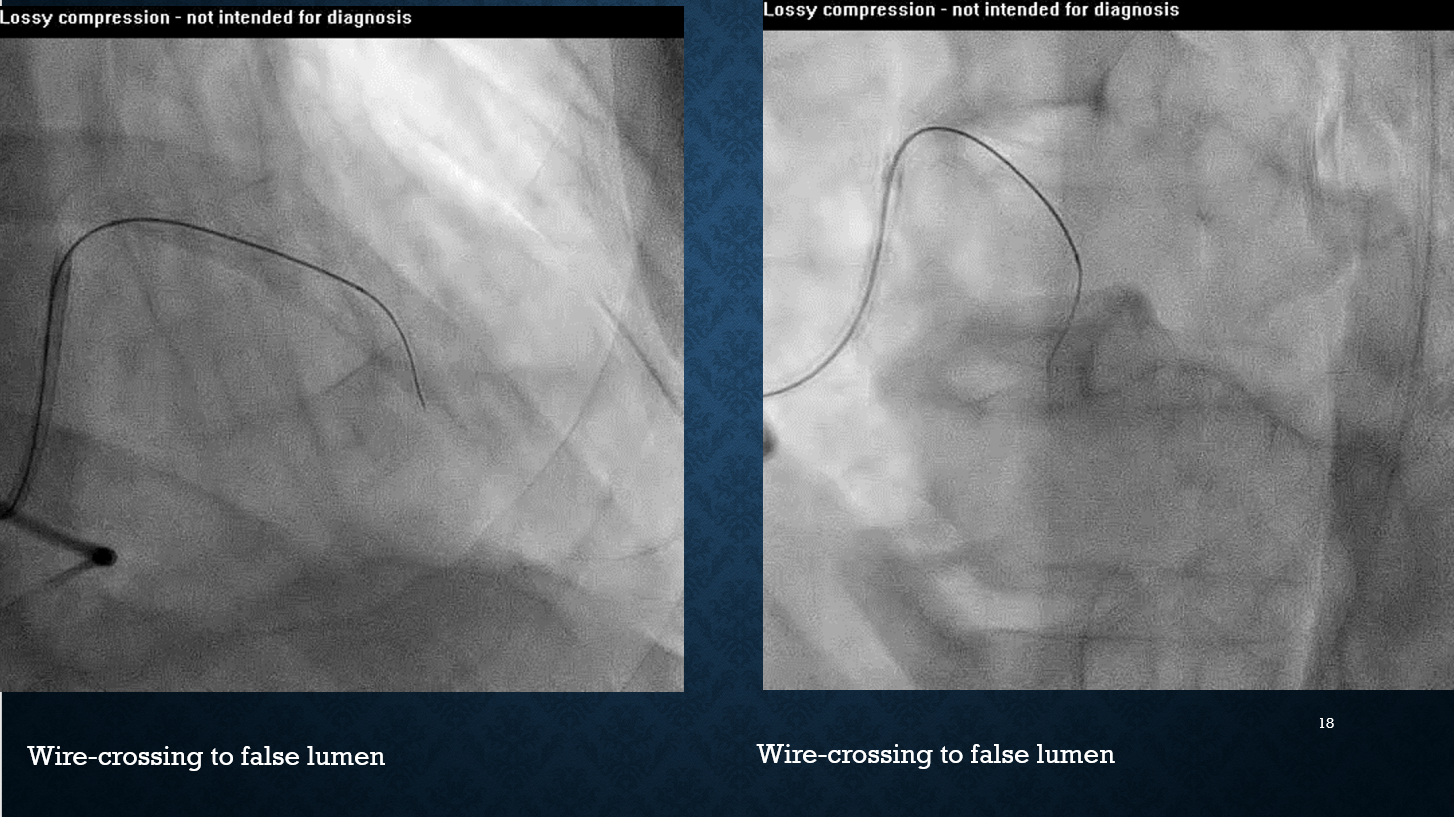
1. Because of relatively difficult fromantegrade approach, we tried retro-grade approach first. We performed contralateralcoronary angiography.


 0506 250 Final.mpg
0506 250 Final.mpg
0506 251 Final.mpg
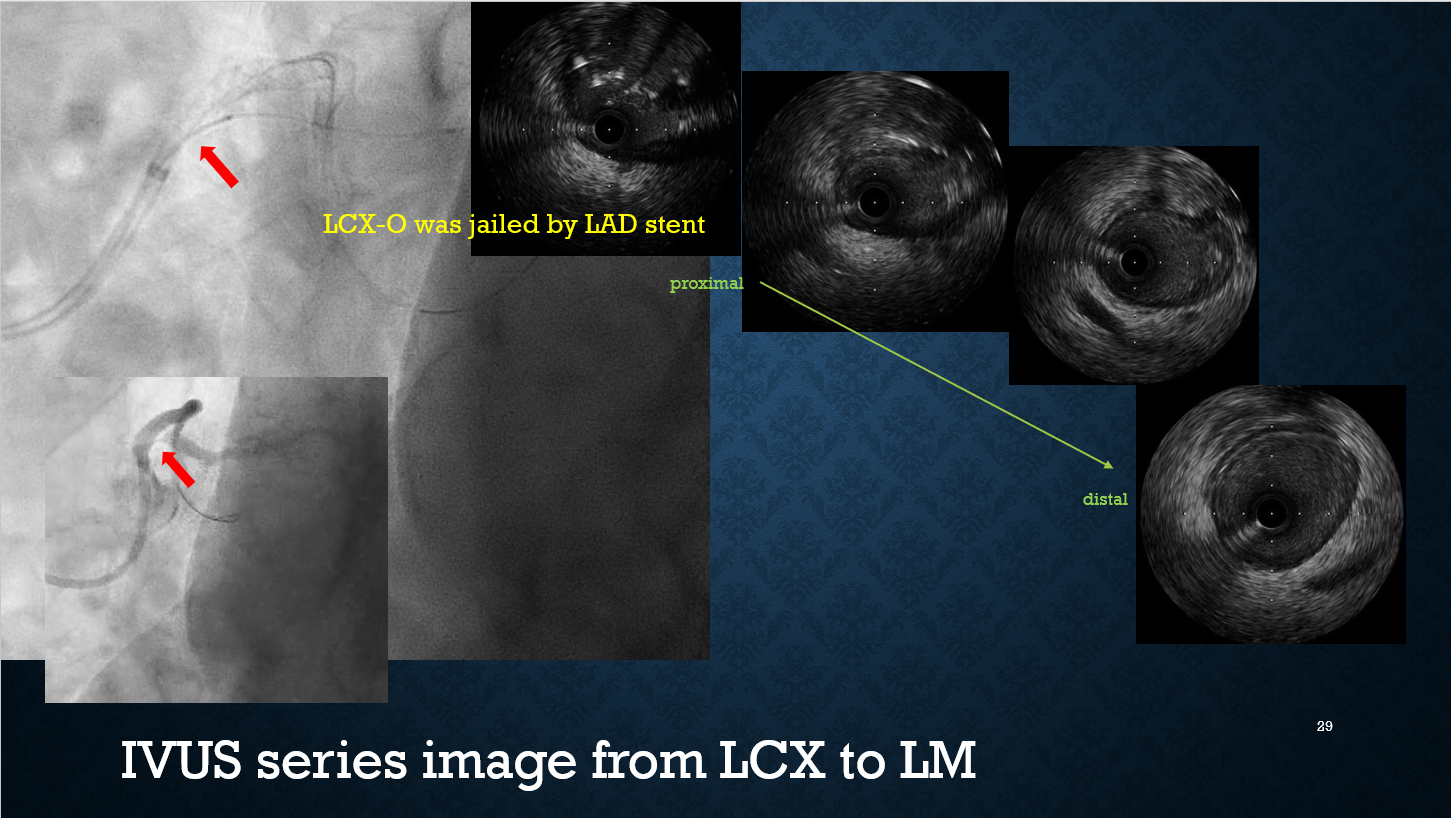
Case Summary
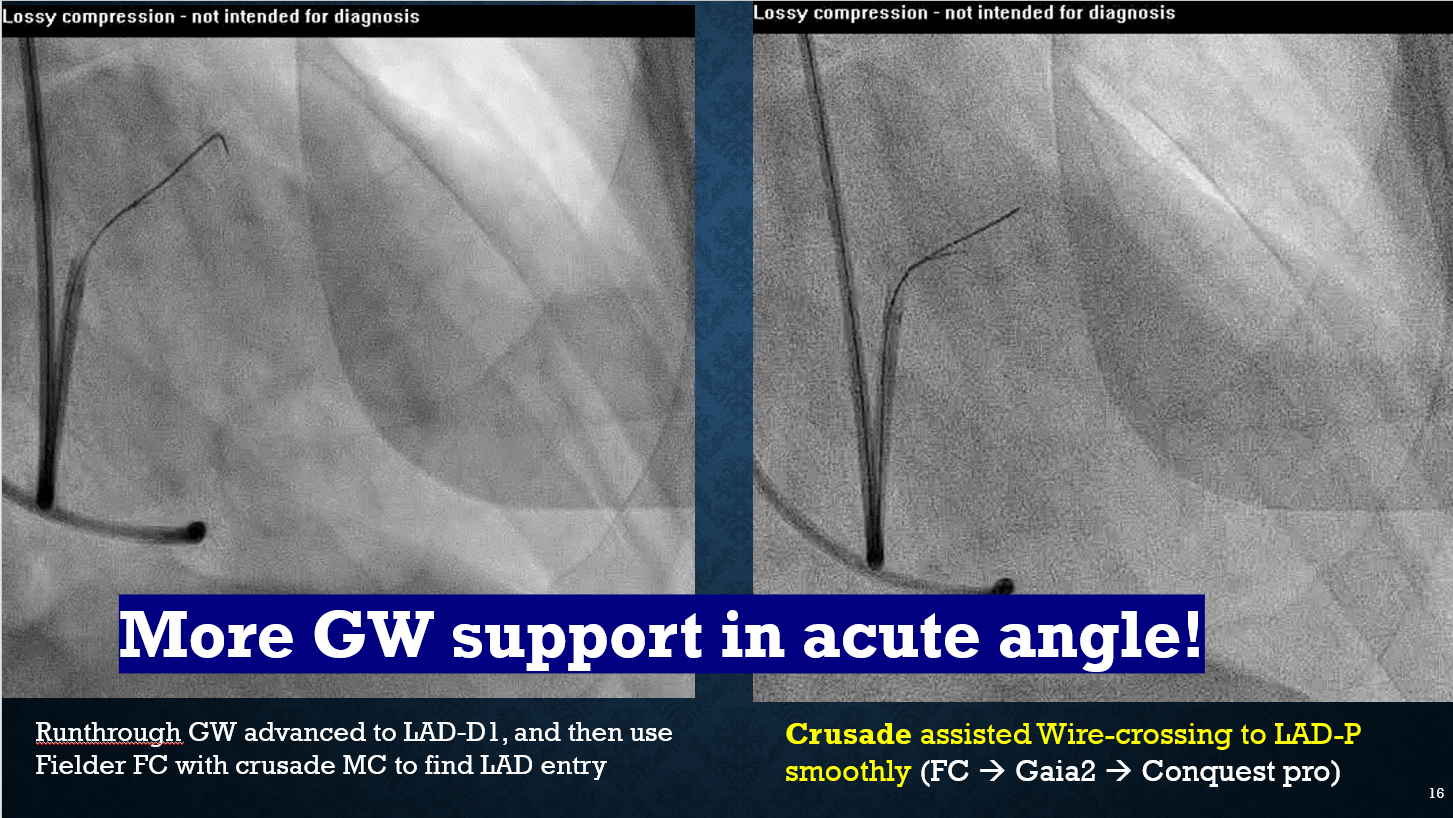
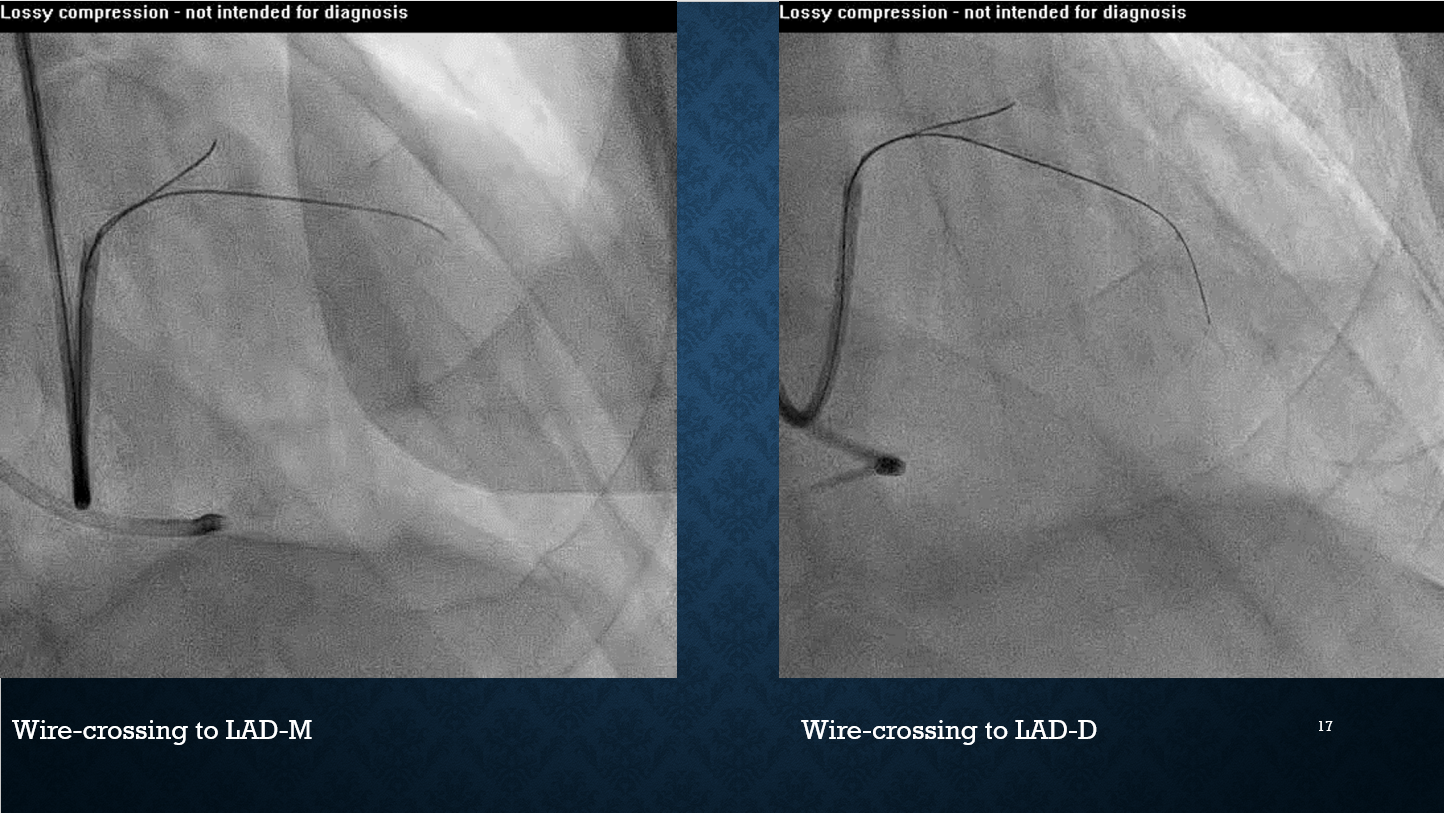
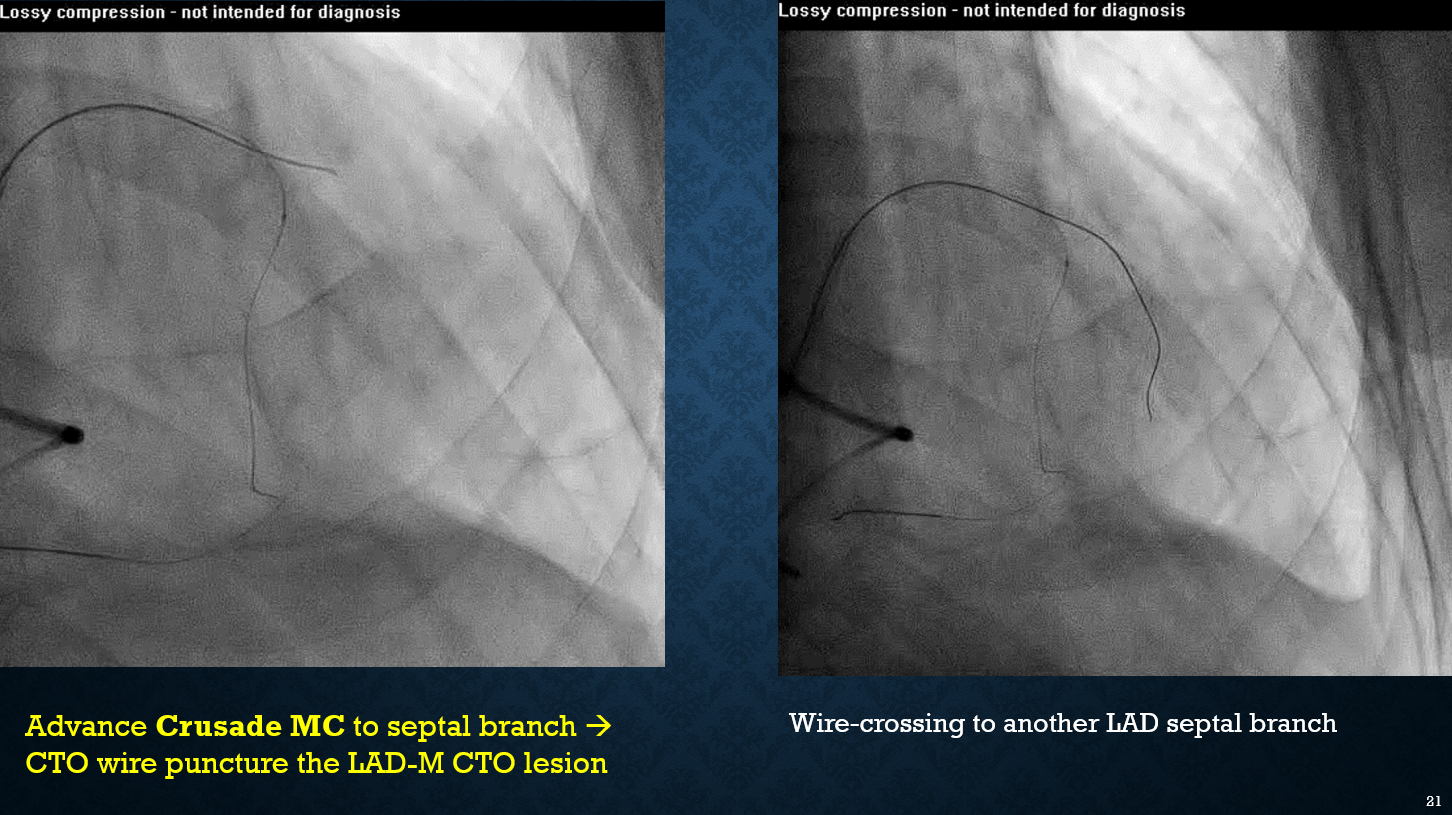
CTO GW with microcatheter support are the basic tools for dealing with CTO lesion. However, long CTO is always difficult, especially when retrograde approach is not available. Crusade microcatheter is often applied for providing antegrade wire support, facilitating wiring of side branches, reverse wire technique, and efficient wiring of stent struts. In this case, we demonstrated a technique for providing antegrade wire support via CTO GW with Crusade MC to pass through a very long LAD CTO lesion (> 6cm) successfully and smoothly. The technique by Crusade microcatheter may has the potential to became standard technique for dealing with the LAD very long CTO lesion.