
CASE20210715_002
"I'll See You At The Crossroads." - A Case of T- Stenting and Protrusion for Left Main MEDINA 1,1,1 Bifurcation Lesion in a Patient with High Bleeding Risk and Balloon Assisted Tracking of Extension Catheter in a Calcified Lesion
By , , , ,
Presenter
Mugilan Sundarajoo
Authors
1, 1, 1, 1, 1
Affiliation
, Malaysia1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
"I'll See You At The Crossroads." - A Case of T- Stenting and Protrusion for Left Main MEDINA 1,1,1 Bifurcation Lesion in a Patient with High Bleeding Risk and Balloon Assisted Tracking of Extension Catheter in a Calcified Lesion
1, 1, 1, 1, 1
, Malaysia1
Clinical Information
Patient initials or Identifier Number
57035
Relevant Clinical History and Physical Exam
This is a 82 years old who initially presented with angina. His co- morbids are Type 2 diabetes mellitus, chronic kidney disease Stage 3B (eGFR 35) with anemia (hemoglobin 9.1, serum iron- 6.2) hypertension and dyslipidemia. He was transferred to our care for recent anteroseptal myocardial infarction requiring intravenous adrenaline. Physical examination revealed bibasal crackles with reduced air entry on the left with no pedal oedema. Cardiac auscultation revealed dual rhythm with no murmur.
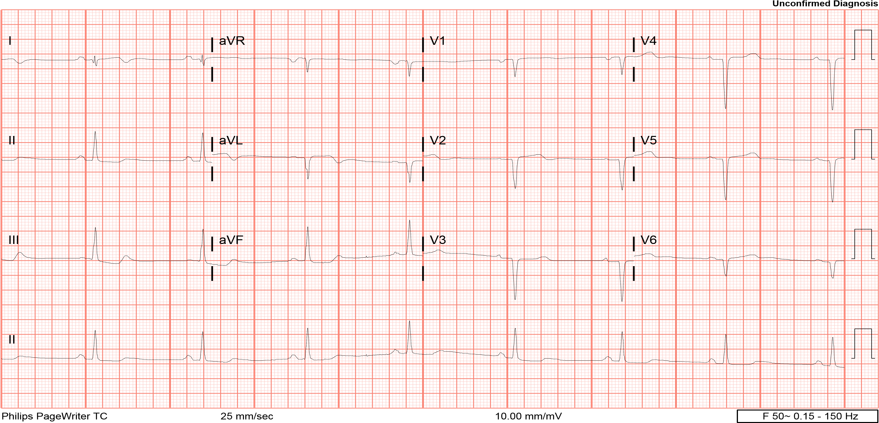
Relevant Test Results Prior to Catheterization
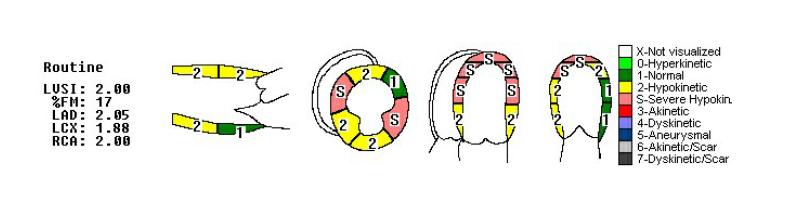
Chest X-ray revealed cardiomegaly with left pleural effuion. ECG showed T inversions over I and aVL with Q waves over anterior leads. 2-D Echocardiography showed concentric left ventricle hypertrophy with ejection fraction of 30 % with Grade 2 diastolic dysfunction and mild mitral regurgitation. Troponin T was unremarkable.

Relevant Catheterization Findings
Left Main Stem - Bifurcation lesion involving the Distal Left
Main Stem (severe disease) - MEDINA 1,1,1 lesion
Left Anterior Descending - Critical ostial disease and severe stenosis over proximal segment
Left Circumflex - Critical ostial stenosis and mild disease at mid-segment
Right Coronary Artery - Mild disease at proximal Right Coronary Artery
Intraaortic balloon pump inserted in view of poor left ventricular function in cardiogenic shock keeping in mind for complex bifurcation stenting.
Interventional Management
Procedural Step
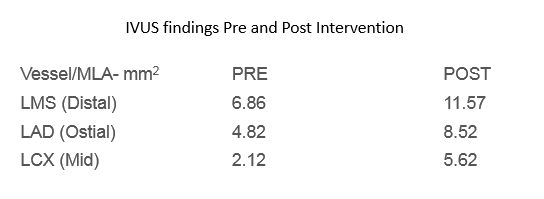
IVUS guided Coronary Angiogram and Angioplasty (T Stenting and Protrusion) LAD - LCX into LMS with Intraaortic Balloon Pump support.7 FR EBU 3.5 Guiding catheter used.Predilatation over distal LMS to ostial LAD done with Sapphire II PRO 1.5 x 12mm at 12 atmPredilation of LCx with Sapphire II PRO 1.5 x 15mm at 12 atm Synergy (DES) stent 2.5 x 20 mm deployed at LCX at nominal pressure with minimal protrusion into Left main stem.Both LAD and LCX prepared further with NC Emerge 2.5 x 15mm in LCX up to 12atm and NC emerge 2.5 x 15 mm up to 16 atm in LADDistal left main had non flow limiting Type B DissectionGuidezilla 6FR used to provide extra support for further intervention to the LAD. The guide extension catheter was delivered down to LAD via balloon assisted tracking technique (BTT)Synergy (DES) stent 2.75 x 28 mm deployed at LAD at nominal pressureSubsequently, further dilatation with NC Emerge 3.0 x 12 mm up to 14 atm to the LADfollowed by NC Trek 2.75 x 12 mm to the Left Circumflex up to 24 atmOstium Diagonal 1 had stenosis due to plaque shift which required multiple predilatation with Kissing balloon inflation (KBI) Proximal optimization technique performed in LMS with NC Emerge 4.5 x 8mm up to 8 atmKBI done with Sapphire II Pro 3.0 x 15mm at LAD up to 14 atm then NC Trek 2.75 x 15mm at LCX at 20 atmRe-POT done with NC Emerge 4.5 x 8 mm was used across LMS - LAD
Good final result, TIMI 3 flow, no immediate complications.IVUS shows good expansion, apposition and no dissection.
 tracking.avi
tracking.avi
pung 5.avi
Good final result, TIMI 3 flow, no immediate complications.IVUS shows good expansion, apposition and no dissection.
Case Summary
Although CABG is considered as gold standard for treatment of left main stem stenosis, particularly bifurcation lesion involving distal left main, there is increasing evidenceto support the use of angioplasty with stenting. T stenting with protrusion was used in view of the bifurcation angle (approximately 90 degrees) between LMS/LAD and LCX. This technique may be practical keeping in mind that higher bifurcation angles are associated with increased rates of adverse events and side branch closure. "Balloon assisted tracking technique" (BTT) proves to be an efficient method for the delivery of guide extension catheter despite the calcified lesion while minimizing vessel injury.