
CASE20210710_001
Percutaneous Coronary Intervention on Unprotected Left Main Coronary Artery Quadfurcation
By , , ,
Presenter
Bryan Rene Toledano
Authors
1, 1, 1, 1
Affiliation
, Philippines1
Complex PCI - Bifurcation/Left Main Diseases and Intervention
Percutaneous Coronary Intervention on Unprotected Left Main Coronary Artery Quadfurcation
1, 1, 1, 1
, Philippines1
Clinical Information
Patient initials or Identifier Number
RR
Relevant Clinical History and Physical Exam
A 66 year old male admitted due to heart failure symptoms. He is a known hypertensive with 10-pack smoking history. On physical examination he had stable vital signs, adynamic precordium, apex beat at 5th left intercostal space anterior axillary line, no murmurs and vesicular breath sounds were noted.
Relevant Test Results Prior to Catheterization
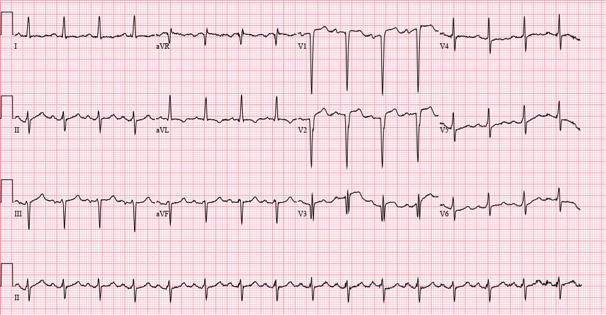
His 12 LECG showed normal sinus rhythm with non specific ST-T wave changes. His HS-troponin I (24.3 pg/ml), Creatinine (1.46mg/dl), and Cystatin C (1.57mg/L) were all elevated. A two dimensional echocardiogram showed an eccentric left ventricular hypertrophy, global hypokinesia with an ejection fraction of 30% by Simpsons.
Relevant Catheterization Findings
The Left Main is a 5mm sized vessel that has 90% distal segment stenosis that quadfurcates into the LAD, RI1, RI2 and LCX. The LAD is a 5mm type III vessel that has sequential 90% ostial, 70% proximal, and 70% mid segment stenoses. The RI1 is a 2.5mm vessel that has 70% ostial stenosis while RI2 is a 1.75mm vessel that has 70% ostial stenosis. The LCX is a 1.75mm non dominant vessel that has 70% ostial stenosis. The RCA is a 5mm dominant vessel that is free of significant disease.
 LAO CAU view.mov
LAO CAU view.mov
RAO CAU view.mov
RAO CRA view.mov
Interventional Management
Procedural Step
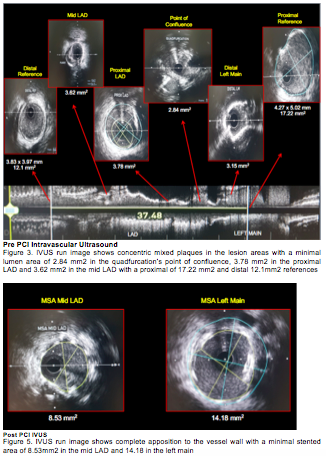
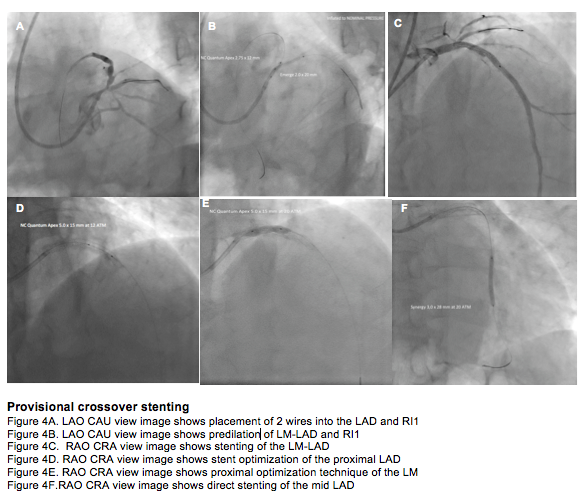
A 6F extra back up catheter 3.5 was used as guide support, coronary guides Asahi Sion blue 0.014 wire was distalized to the LAD & Asahi Sion 0.014 wire to theRI1. Pre dilation using Emerge 2.0 x 20mm PTCA dilation catheter was positioned and inflated in the distal LMCA to proximal LAD at 14 ATM. IVUS run showed concentric plaques in the lesion areas with minimal lumen area of 3.15 mm2 in the LMCA, 3.78 mm2 in the proximal LAD, 3.63 mm2 in the mid LAD with a distal reference area of 12.1 mm2. A kissing balloon predilation using Emerge 2.0 x 20mm PTCA balloon catheter positioned at the distal left main to proximal RI1 and a NC Quantum Apex 2.75 x 20mm PTCA balloon catheter, positioned at the distal left main to proximal LAD were both inflated to nominal pressures. A Synergy 3.0 x 28mm stent was positioned and deployed in the mid left main to mid LAD at 11 ATM. This was followed by post dilation of the proximal to mid stented LAD at 12 ATM and proximal optimization at 20 ATM using NC Quantum Apex 5.0 x 15mm PTCA balloon. A second stent, Synergy 3.0 x 28mm was positioned and deployed in the mid LAD at 20 ATM. A post PCI IVUS showed complete stent apposition to the vessel wall with minimal stented area of 8.53mm2 in the mid LAD and 14.18mm2 in the Left Main. Post PCI angiography showed TIMI flow 3 in all vessels.
LAO CAU view post PCI.mov
Case Summary
A Quadfurcation with two ramus intermedius is a rare anatomic variant that makes stenting more complex. Defining the angle, supply and size of the all side branches are important in choosing which protection strategy is needed. The use of intravascular ultrasound to distinguish a high origin marginal/diagonal branch from a true rams intermedius is accurate. In this kind of case provisional cross over stenting of the Left main to Left anterior descending artery, optimize and guided by intravascular ultrasound may be employed with good angiographic and procedural success.