CASE20240815_005
When the Only Way Is the Most Challenging in a Retrograde CTO PCI
By Ramy Mohamed Atlm, Salma Mohamed Elshokafy
Presenter
Ramy Mohamed Atlm
Authors
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy 1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
CASE20240815_005
Complex PCI - CTO
When the Only Way Is the Most Challenging in a Retrograde CTO PCI
Ramy Mohamed Atlm1, Salma Mohamed Elshokafy 1
Tanta University Hospital, Egypt1,
Clinical Information
Relevant Clinical History and Physical Exam
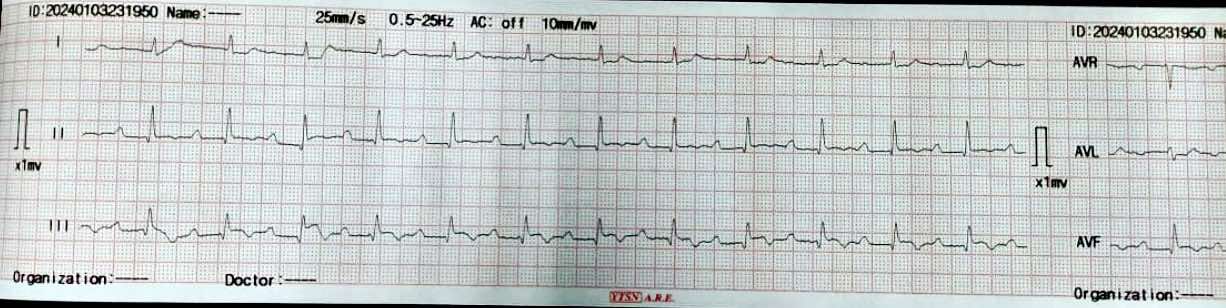
Male patient, 68 years old , Diabetic , Hypertensive .Ischemic heart disease with PCI to LAD 2 years ago .Recurrent chest pain with multiple admissions with ACS during the last 3 months for which coronary angiography was recommended ECG: SR with ST , T changes in inferior leads .ECHO: IHD with EF 52%, RSWMAs in the form of ( apical and Mid inferior and infero-septal wall hypokinesia ) with Moderate mitral valve incompetence BLPR: 140/90 mmHg , HR : 75 B/M , TEMP: 36.2 c , RBS : 258
Relevant Test Results Prior to Catheterization
Coronary angiography was done showing patent previous LAD stent and CTO RCA ** Symptomatic patient ** Good EF with SWMA at RCA territory ** Recurrent admissions with ACS And also Thallium study was done to document Ischemic burden of RCA territory and was positive

Relevant Catheterization Findings
LM : Normal vessel bifurcating into LAD & LCX.LAD : Atherosclerotic vessel with patent previously deployed stent .LCX: A atherosclerotic small diffusely diseased vessel .RCA : Atherosclerotic vessel with proximal CTO with bridging collaterals and retrograde good septal and epicardial collaterals from left system
 Series_001_Coro.wmv
Series_001_Coro.wmv
Series_003_Coro.wmv
Series_004_Coro.wmv
Interventional Management
Procedural Step
Dual femoral access , Dual injection through AL1 7F & XB4 7F Target vessel assessment ( RCA ) with calculation of J-CTO score then deciding which strategy we decided a Trial antegrade, If failed , Retrograde through septals , If failed , shift to epicardial collateral.Antegrade Trial with GAIA Wires , Corsair MC failed , Retrograde trial through septals failed as it seems not connected shifting strategy to epicardial : Sion blue navigated through epicardial collaterals , corsair 150 MC
successfully passed through PL branch MC advanced to distal Cap & GAIA 2nd wire successfully pierced distal cap , but failed to entre antegrade guide Trial snaring through AL guiding by a home made snare but failed , Guiding changed to JR with successful snaring of wire into antegrade guide followed by MCPilot 50 wire introduced through retrograde MC ( Rendezvous Technique , Reverse TIP IN ) then MC Withdrawn we started conventional PCI with Antegrade Balloon dilatation
2.5 * 15 mm semicompliant then 3.5 * 15 mm NC balloons Then stenting with 2 overlapping DES with postdialtation with 4*15 NC balloon with final good angiographic results
Series_007_Coro.wmv
Series_009_FL Card.wmv
Series_043_Coro.wmv
Case Summary
** Assessing CC size is mandatory , as sizable epicardial channel can accommodate corsair MC. ** Snaring and Rendezvous ( TIP IN ) technique can over come challenges during standard wire externalization .** Short wires ( 180 cm ) NEVER be snared , but if it happens the wire should be pulled out from the antegrade guide , without attempting to retrieve it from the retrograde direction .** Keep your mind active and Always be prepared for surprises