CASE20240815_003
"CARLINO" Saving a Retrograde CTO RCA ,, " When You Got Stucked, You Must Find a Way Out "
By Salma Mohamed Elshokafy, Ramy Mohamed Atlm
Presenter
Salma Mohamed Elshokafy
Authors
Salma Mohamed Elshokafy1, Ramy Mohamed Atlm1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
CASE20240815_003
Complex PCI - CTO
"CARLINO" Saving a Retrograde CTO RCA ,, " When You Got Stucked, You Must Find a Way Out "
Salma Mohamed Elshokafy1, Ramy Mohamed Atlm1
Tanta University Hospital, Egypt1,
Clinical Information
Relevant Clinical History and Physical Exam
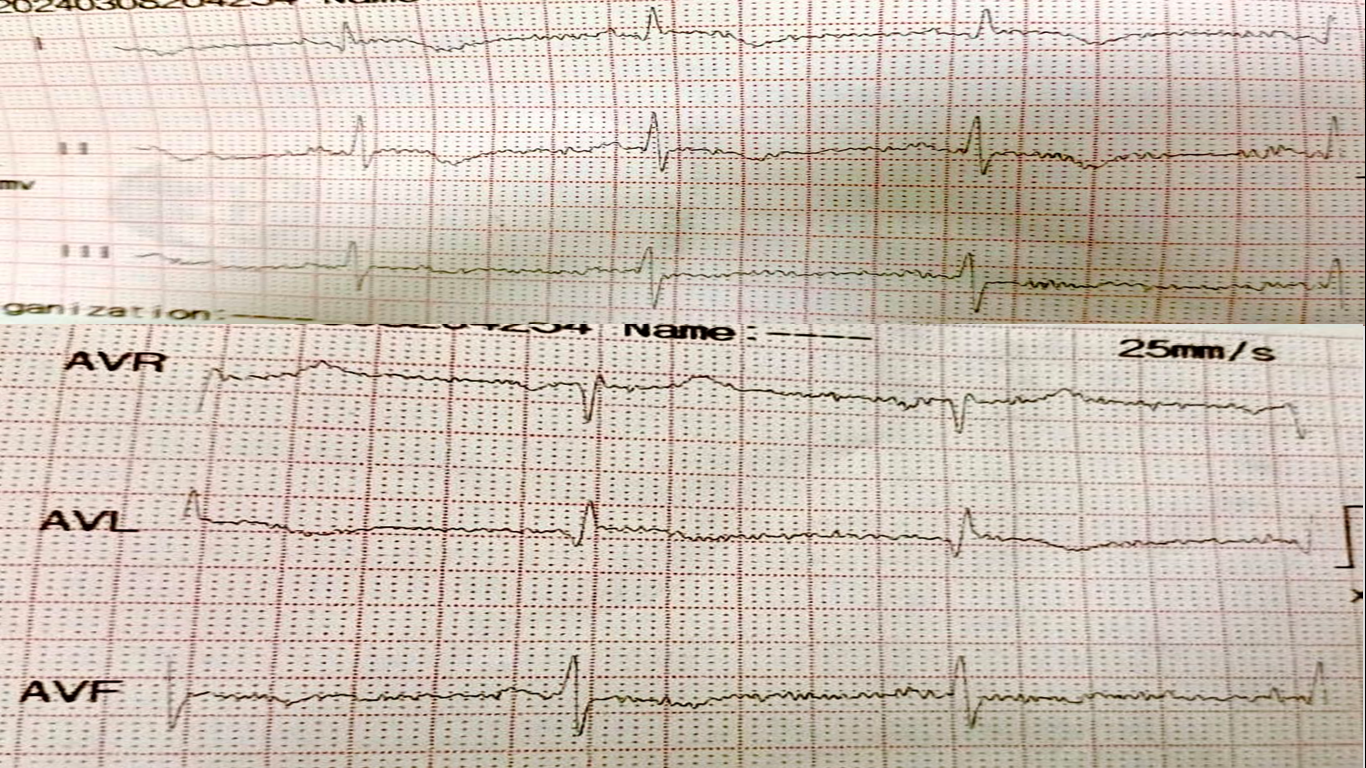
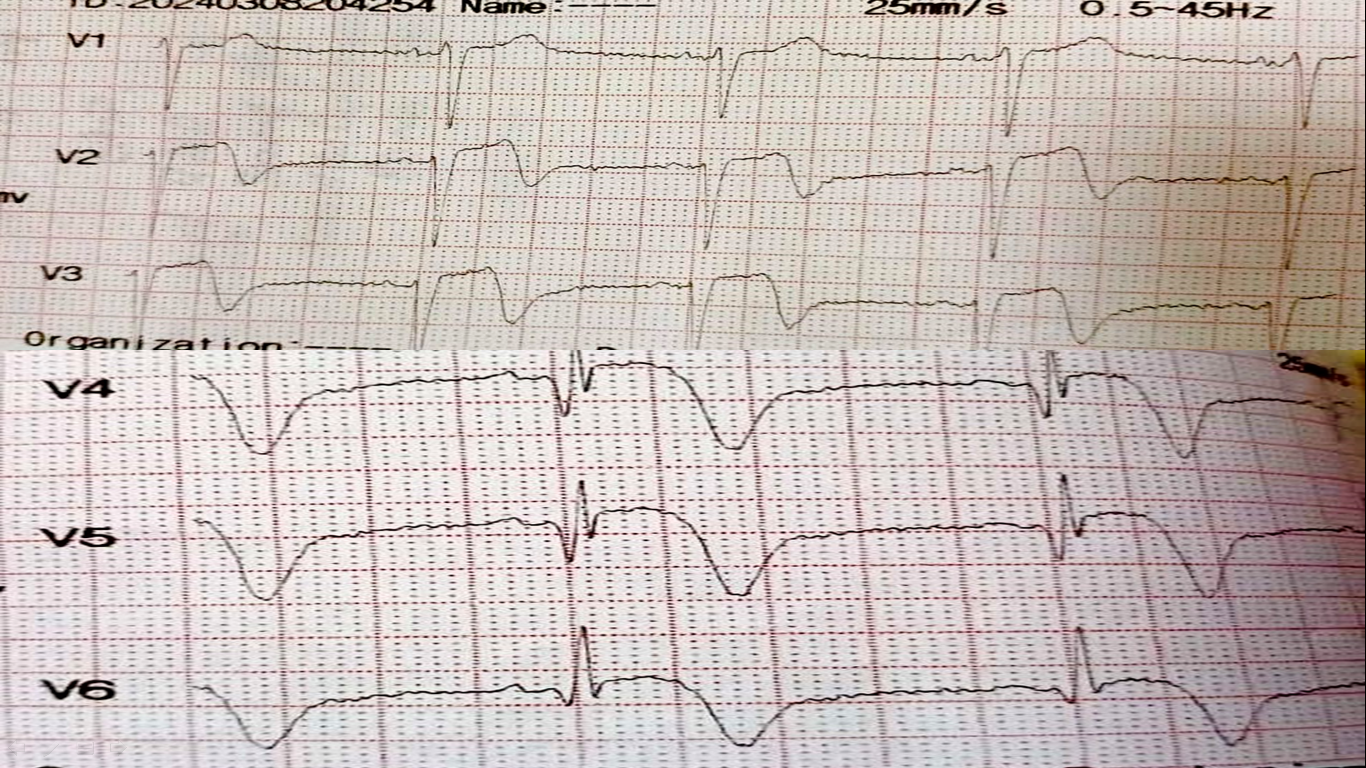
Male patient, 63 years old , Diabetic , Dislipidemic History of extensive anterior STEMI with primary PCI to LAD with one DES & coronary angiography at that time shows CTO RCA . ECG: Normal sinus rhythm with ( old anterior STEMI ) and T wave inversion in inferior leads ECHO : Ischemic heart disease with RSWMA and EF 48 %BLPR: 130 / 80 mmHg , HR: 85 B/M , TEMP : 37 c , RBS 300
Relevant Test Results Prior to Catheterization
Thallium study done showing ischemic viable myocardium at RCA territory

Relevant Catheterization Findings
LM : Normal vessel bifurcating into LAD & LCXLAD : Atherosclerotic vessel with patent previously predeployed stent LCX : Atherosclerotic vessel with no significant lesions RCA : Atherosclerotic vessel with midsegment CTO receiving retrograde good septal & epicardial collaterals
 Series_002_Left Coronary 15 fps.wmv
Series_002_Left Coronary 15 fps.wmv
Series_003_Left Coronary 15 fps.wmv
Series_006_Left Coronary 15 fps.wmv
Interventional Management
Procedural Step
First we assessed Target vessel : RCA., Calculate J-CTO score & Select strategy of PCI which was trial antegrade if failed we will go through retrograde approach via septal collaterals .Bi Femoral access , Dual Injection was done through JR 4 6F and EBU 4 6F.BMW wire in LAD , Another one through septal collaterals with Corsair pro MC then Sion blue for surfing >> Failed .Selective injection showed Connected channel so wire changed to Sion Black .MC reaches distal cap then RWE ( Fielder XTA Pilot 150 GAIA 3rd ) with Failure to penetrate the distal cap >> dissection.Tip injection from MC at distal cap Seems it was extraplaque Modified from dye injection , so we shifted to RDR via Dye based CARLINO.Pilot 150 reentered true lumen followed by MC that stucked at another CTO level. We changed MC to CARAVEL then , Again RWE ( Fielder XTA GAIA 2nd , 3rd Pilot 150 ) Succeeded to entre true lumen .From true lumen to antegrade guide followed by MC , then trapped and externalization was done with RG3 followed by conventional PCI steps .Antegrade Balloon dilatation with 2.5 * 20 mm semi compliant balloon .Stenting of RCA from osteal to distal with 3 DES followed by postdilatation and flaring with final good angiographic results.
Series_014_Left Coronary 15 fps.wmv
Series_017_Left Coronary 15 fps.wmv
Series_045_Left Coronary 15 fps.wmv
Case Summary
To summarize First Stuck : When SION BLUE wire failed to cross collaterals may be due to tiny caliber or acute angle of entry so exchanged with SION BLACK .Second Stuck: When we go through first CTO level with RWE that failed and shifted RDR through CARLINO technique " inject minimal amount 0.5 mm dye to modify plaque " . Third Stuck : When CORSAIR MC failed to cross the second CTO level and changed to CARAVEL .Fourth Stuck : At second CTO level RWE failed so shifted to RDR .Finally ,,You should put a strategic plan , But also you should be prepared to change the strategy at any time .Managing different techniques and modalities usually ends by procedural success.