CASE20241016_004
Cracking the Calcium Chunk: Successful Management of Heavily Calcified Left Main Bifurcation Lesions
By Soo Yeon An
Presenter
Soo Yeon An
Authors
Soo Yeon An1
Affiliation
Asan Medical Center, Korea (Republic of)1,
View Study Report
CASE20241016_004
Complex PCI - Left Main
Cracking the Calcium Chunk: Successful Management of Heavily Calcified Left Main Bifurcation Lesions
Soo Yeon An1
Asan Medical Center, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
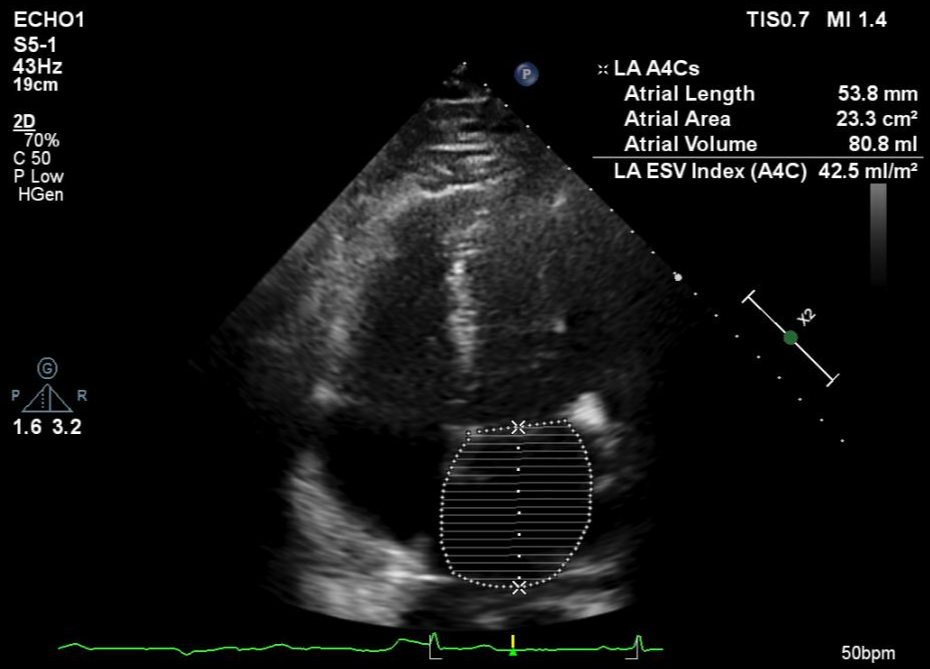
A 76-year-old male with a past medical history of hypertension presented with effort-induced chest discomfort. He reported experiencing chest pain over the past 2 months, particularly when walking or ascending an incline. The chest pain, located in the left precordium, was described as tight and squeezing, lasting less than one minute. Echocardiography showed the left atrial enlargement and normal LV systolic function without definite regional wall motion abnormality (Figure 2-1).
Relevant Test Results Prior to Catheterization
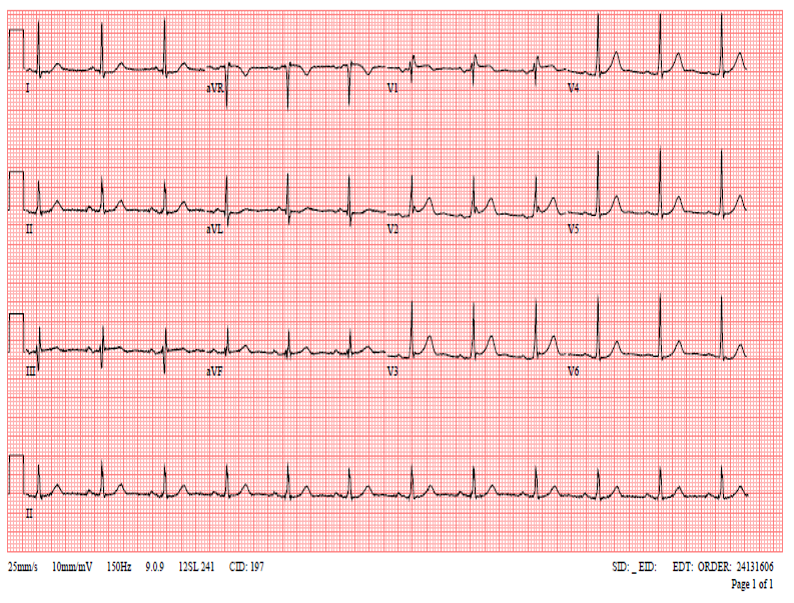
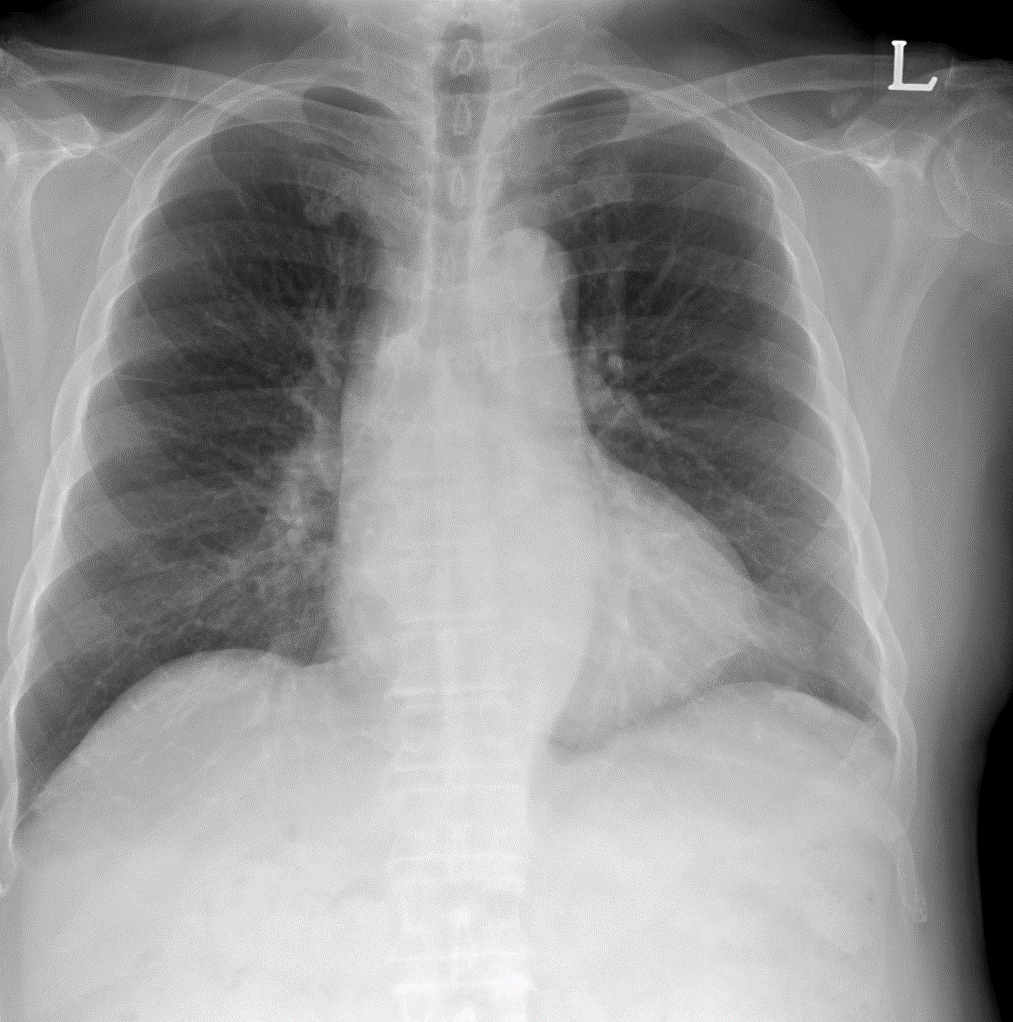
ECG: ECG showed a normal sinus rhythm with a heart rate of 56 bpm. No significant arrhythmias or conduction abnormalities were reported (Figure 3-1).Chest X-ray: there were no findings to suggest cardiomegaly, pulmonary congestion, or pleural effusions (Figure 3-2).
Relevant Catheterization Findings
Right Coronary Artery (RCA): Diffuse 80% stenosis (>20 mm) (Video 4-1).LM bifurcation: 90% stenosis, B1 type lesion, 10-20 mm in length (Video 4-2).LAD ostium: up to 99% stenosis, B2 type lesion, subtotal occlusion.LCX ostium: up to 99% stenosis, B2 type lesion, subtotal occlusion (Video 4-3).
 4-1_RCA.avi
4-1_RCA.avi
4-2_CAU.avi
4-3_SPIDER.avi
Interventional Management
Procedural Step
The PCI procedure began with the insertion of a 7-French JL4 guiding catheter with a side hole via Rt. Femoral approach. Rotablator burrs of 1.5mm and 1.75 mm were used to modify calcified plaques from the LM to the proximal LAD and the LCX ostium(Video 5-1). After pre-dilation, IVUS was performed in both the LAD and LCX. Xience Skypoint 3.5×15mm stent was delivered to the LCX and deployed from the LM to the proximal LCX, followed by post-dilatation with a Selethru 3.5×10mm balloon up to 24 atm. The LCX stent was then crushed by deploying a second DES (Xience Skypoint 3.0×38mm) from the LM into the proximal LAD. Post-dilatation of the LAD stent was performed with Raiden3 3.25×15mm at the distal edge and Selethru NC 4.0×10mm balloons. Rewiring into the LCX stent was challenging, requiring the exchange to a Fielder XT-R wire(Video 5-2). The initial attempt to pass a Selethru 3.5×10mm balloon through the angled LCX ostium failed. Dilations were performed with Ryurei 1.5×15mm and 2.0×15mm balloons. The first kissing balloon inflation was done, using Selethru NC 3.5×10mm in the LAD and Across HP 3.5×15mm in the LCX at 10 atm. Post-dilatation followed with Selethru NC 4.0×10mm and 4.5×10mm balloons from the LM to the proximal stent edges. The LCX was re-wired and a second kissing balloon inflation was performed using Selethru NC 4.5×10mm in the LAD and 4.0×10mm in the LCX. After the final kissing balloon inflation, the procedure achieved excellent angiographic results(Video 5-3).
5-1_Rotablation.avi
5-2_Rewire LCX.avi
5-3_Final.avi
Case Summary
In this case, the treatment strategy involved PCI using an upfront two-stent approach for significant LM bifurcation disease, facilitated by rotational atherectomy to address heavily calcified lesions. Post-dilatation and a final kissing balloon inflation at the LM-LCX bifurcation were performed to ensure full stent expansion and apposition. IVUS was used to guide the procedure, ensuring precise stent placement and minimizing the risk of malapposition, optimizing the overall outcome.