CASE20240928_001
A Challenging Case Report: How to Overcome Disconnection of the Burr from the Drive Shaft During Rotational Atherectomy of a Very Tortuous and Calcified In-Stent Restenosis Lesion
By Seunghan Lee, Kyeongwon Seo, Hansu Park, Seongbong Wee, Sooyeon Ahn, Do-Yoon Kang, Jung-Min Ahn, Duk-Woo Park, Seung-Jung Park
Presenter
Seunghan Lee
Authors
Seunghan Lee1, Kyeongwon Seo1, Hansu Park1, Seongbong Wee1, Sooyeon Ahn1, Do-Yoon Kang1, Jung-Min Ahn1, Duk-Woo Park1, Seung-Jung Park1
Affiliation
Asan Medical Center, Korea (Republic of)1,
View Study Report
CASE20240928_001
Complex PCI - Calcified Lesion
A Challenging Case Report: How to Overcome Disconnection of the Burr from the Drive Shaft During Rotational Atherectomy of a Very Tortuous and Calcified In-Stent Restenosis Lesion
Seunghan Lee1, Kyeongwon Seo1, Hansu Park1, Seongbong Wee1, Sooyeon Ahn1, Do-Yoon Kang1, Jung-Min Ahn1, Duk-Woo Park1, Seung-Jung Park1
Asan Medical Center, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
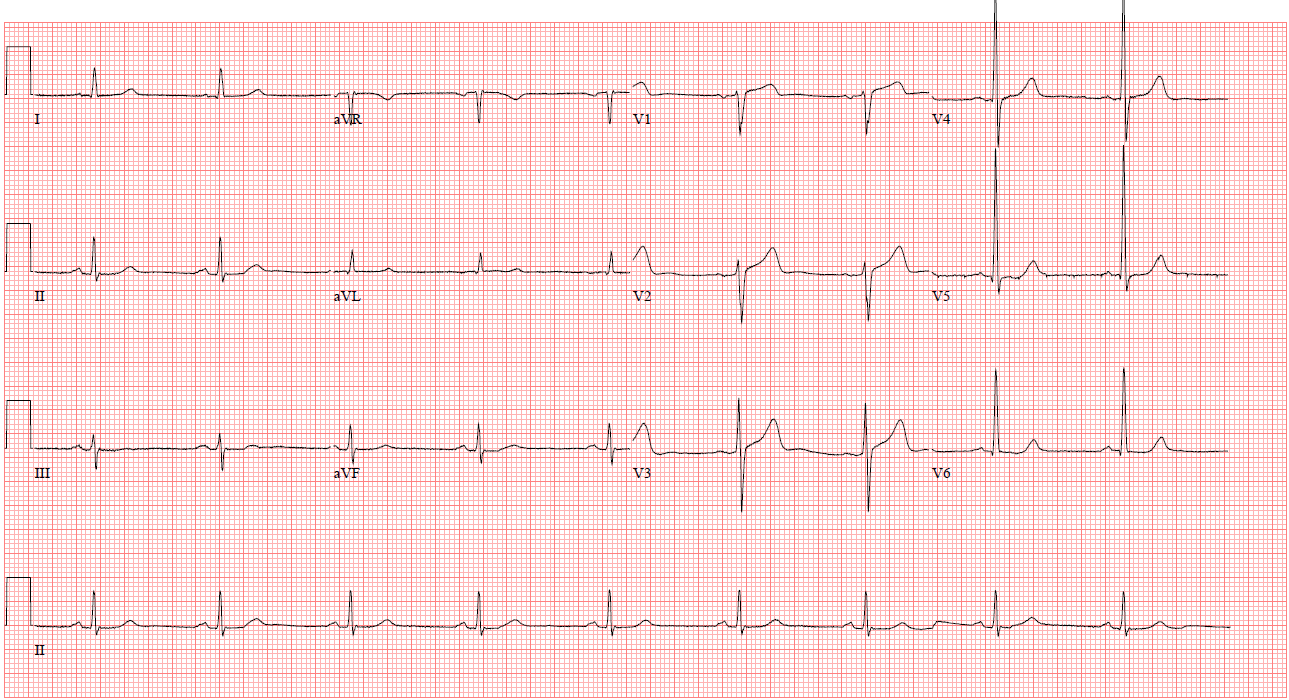
The patient is a 78-year-old male who has been taking oral medication for diabetes for the past 40 years. He has a history of unstable angina and underwent percutaneous coronary intervention from the left main coronary artery to the mid left anterior descending artery 11 years ago, and from the mid to distal right coronary artery 9 years ago. He presented with effort-related chest pain that started one month ago. A chest X-ray showed no significant lesion, and the EKG showed normal sinus rhythm.
Relevant Test Results Prior to Catheterization
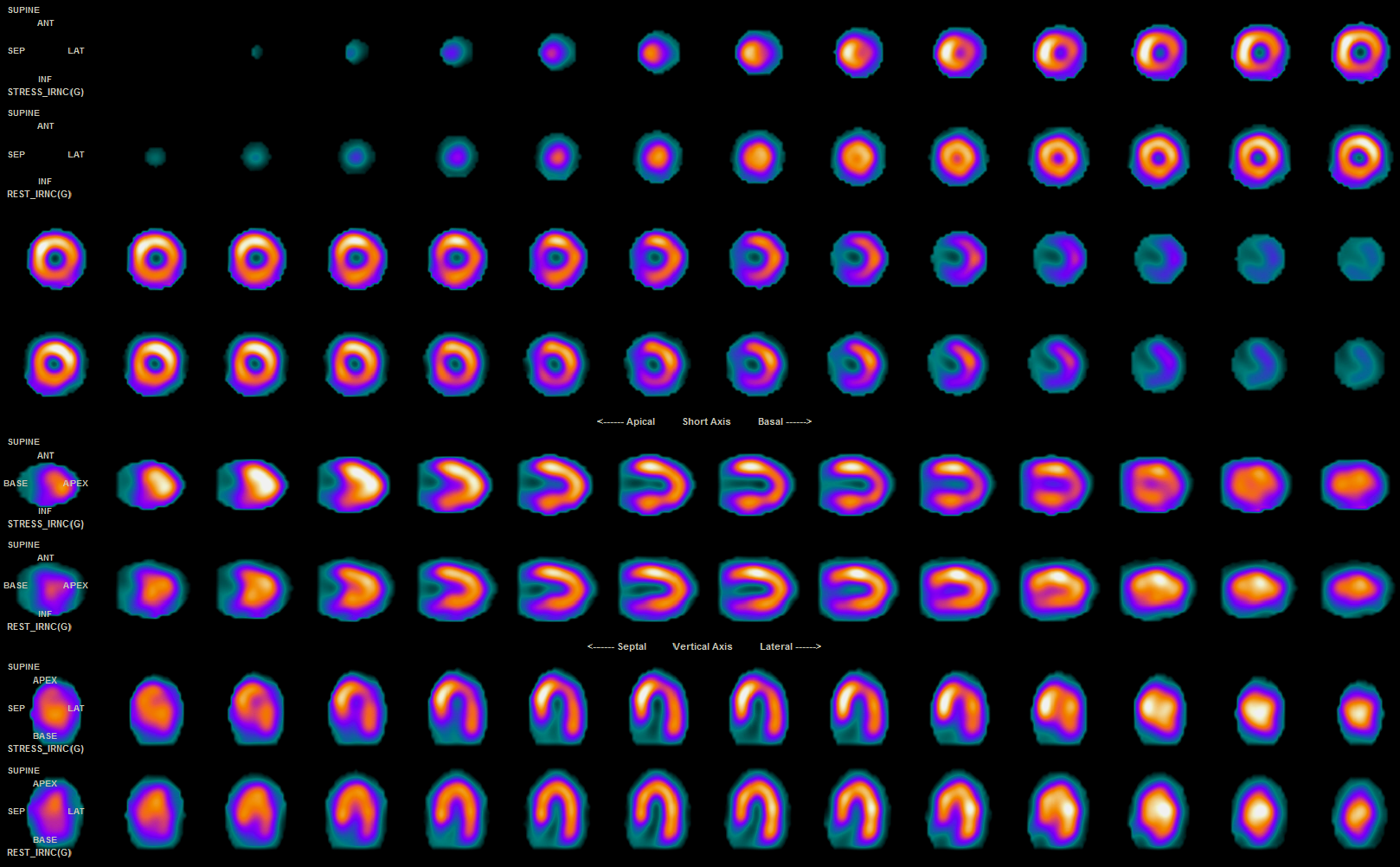
The echocardiogram showed normal left ventricular function with no regional wall motion abnormalities. To assess the presence of ischemia, a myocardial thallium SPECT scan revealed a reversible perfusion defect in the anterolateral and inferolateral walls, prompting the planning of a coronary angiography.
 TTE1-preA4C.mp4
TTE1-preA4C.mp4
Relevant Catheterization Findings
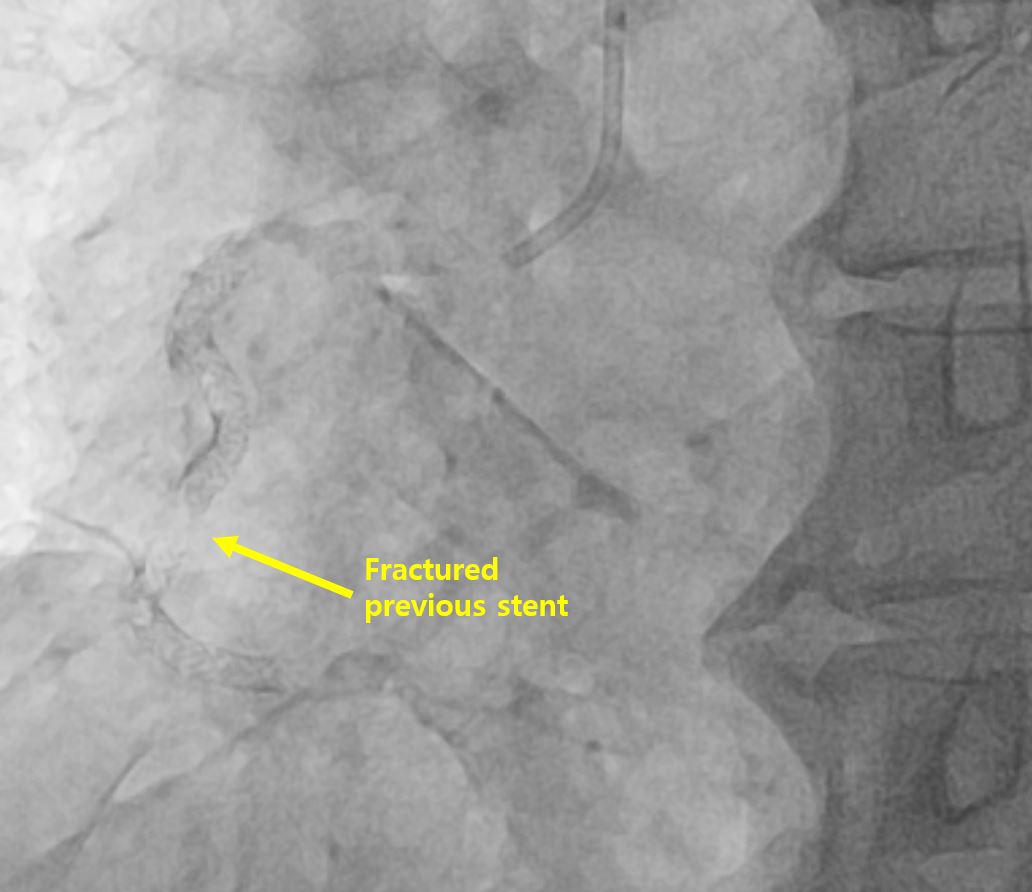
9 years ago, stents were overlapped in the mid to distal RCA. Due to a heavily tortuous and calcified lesion, post-dilation resulted in stent fracture and migration, creating a gap between the stents. A diagnostic coronary angiography was performed, revealing severe stenosis at the site of the stent fracture in the mid RCA, with progression of calcification as well. FFR was done, and during hyperemia, it decreased to 0.70, leading to the planning of PCI that included rotational atherectomy.
CAG1-2015 RCA final.mp4
CAG2-preRCA1.mp4
Interventional Management
Procedural Step
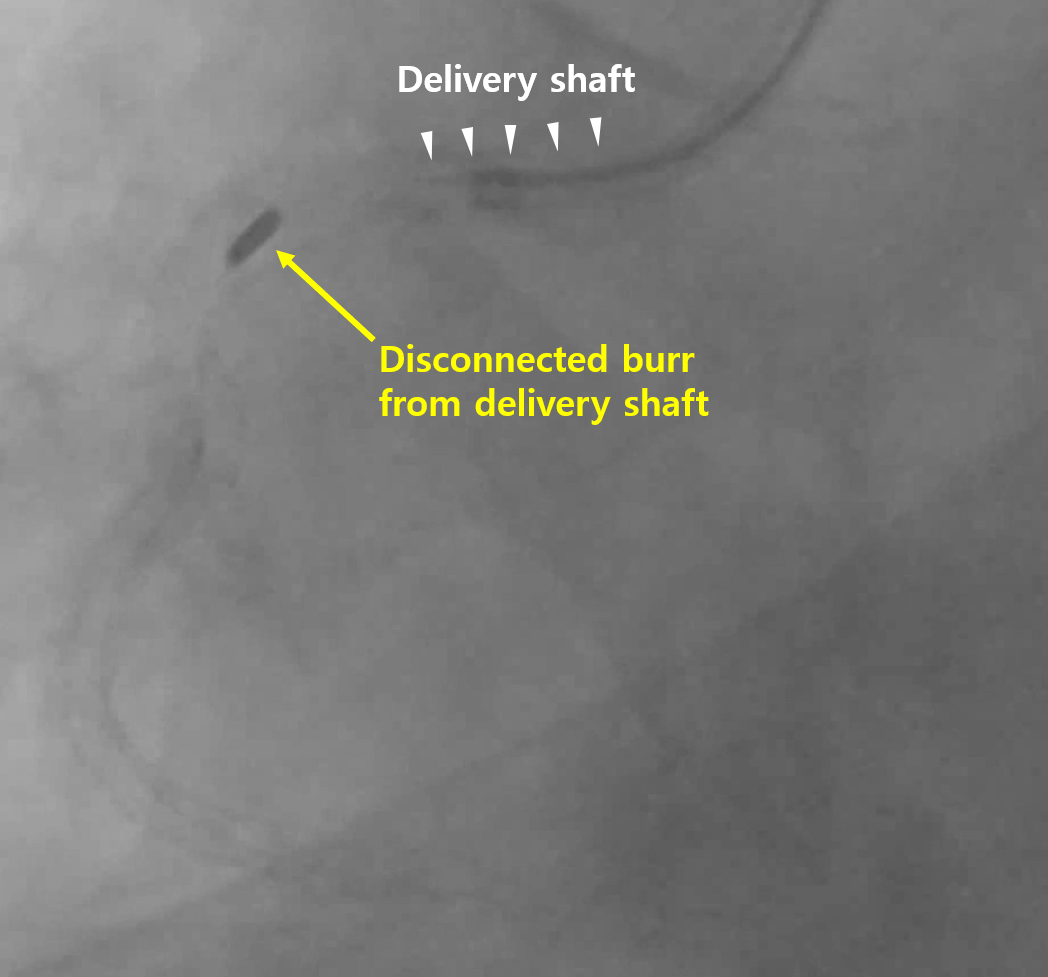
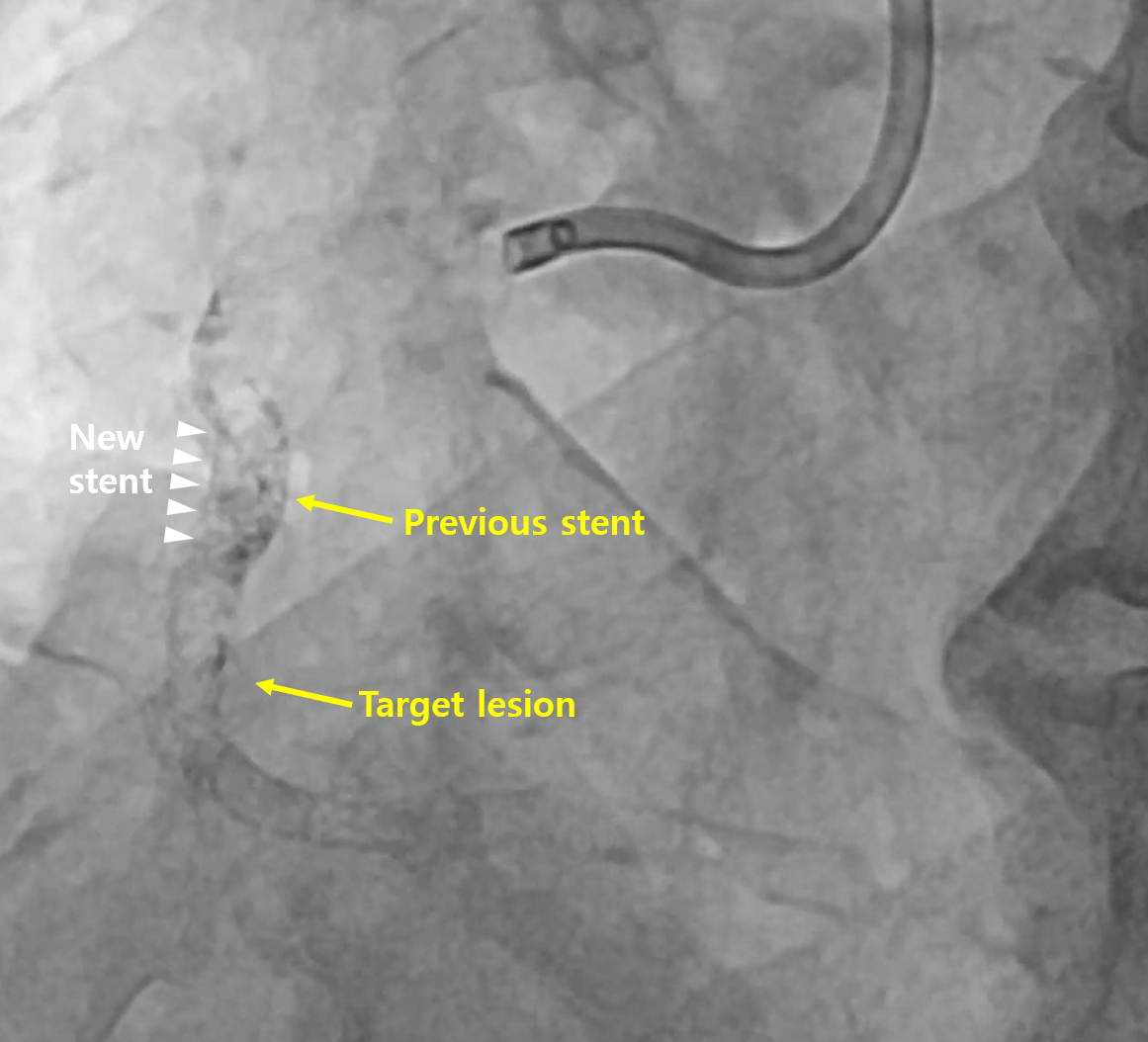
After puncturing the right radial artery, a 6 Fr Judkin 4 right guiding catheter was used. A Sion wire, along with a 6 Fr Guide Liner Guide Extension Catheter and a Caravel Micro-Guide catheter, was utilized to pass the Rotawire into the right coronary artery. Rotational atherectomy was performed on the calcified lesion in the proximal to mid RCA using a 1.25 mm burr. During the procedure, the burr became stuck and disconnected from the drive shaft. The shaft was advanced and retracted once more, and fortunately, the stuck burr was able to be retrieved proximally. Afterward, the burr was gently retracted into the guiding catheter to ensure it was not left in the coronary artery or aorta. The entire system, including the Rotawire, advancer, and guiding catheter, was then removed simultaneously from the right radial sheath.The right femoral artery was re-punctured, and an 7 Fr Amplatz left 1 guiding catheter was used. The mid RCA target lesion with severe stenosis did not adequately dilate despite predilation, as the proximal segment of the target lesion was very tortuous and calcified, successful stent delivery was failed. After confirming sufficient luminal size with IVUS, it was decided to create a new path by penetrating the previous stent strut. Rotational atherectomy was performed on the previous strut and the calcified lesion, and successfully the stent insertion in mid RCA new path was done.
CAG4-entire system removal.mp4
Case Summary
This case involved a patient with a heavily tortuous and calcified in-stent restenosis lesion who had suffered from diabetes for a long time, in which we attempted rotational atherectomy and successfully overcame a situation where the stuck burr became disconnected from the drive shaft. Typically, if a disconnection or shaft fracture occurs, methods such as snaring, surgery, or conservative approaches are employed to overcome the issue. In this case, to prevent the burr from remaining within the vessel, we simultaneously removed the entire system, including the Rotawire, advancer, and guiding catheter. This approach allowed us to safely extract the burr without leaving it in the vessel.