CASE20240927_001
Successful Rotablation in a Highly Tortuous and Heavily Calcified Coronary Lesion During PCI
By Jung-Min Ahn, Seong-Bong Wee, Seung-Jung Park
Presenter
Seong-Bong Wee
Authors
Jung-Min Ahn1, Seong-Bong Wee1, Seung-Jung Park1
Affiliation
Asan Medical Center, Korea (Republic of)1,
View Study Report
CASE20240927_001
Complex PCI - Calcified Lesion
Successful Rotablation in a Highly Tortuous and Heavily Calcified Coronary Lesion During PCI
Jung-Min Ahn1, Seong-Bong Wee1, Seung-Jung Park1
Asan Medical Center, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
A 75-year-old man presented with dyspnea on exertion despite optimal guideline-directed medical therapy. Notably, he had a history of percutaneous coronary intervention (PCI) at the proximal left anterior descending artery (LAD) and obtuse marginal artery (OM) in 2004.

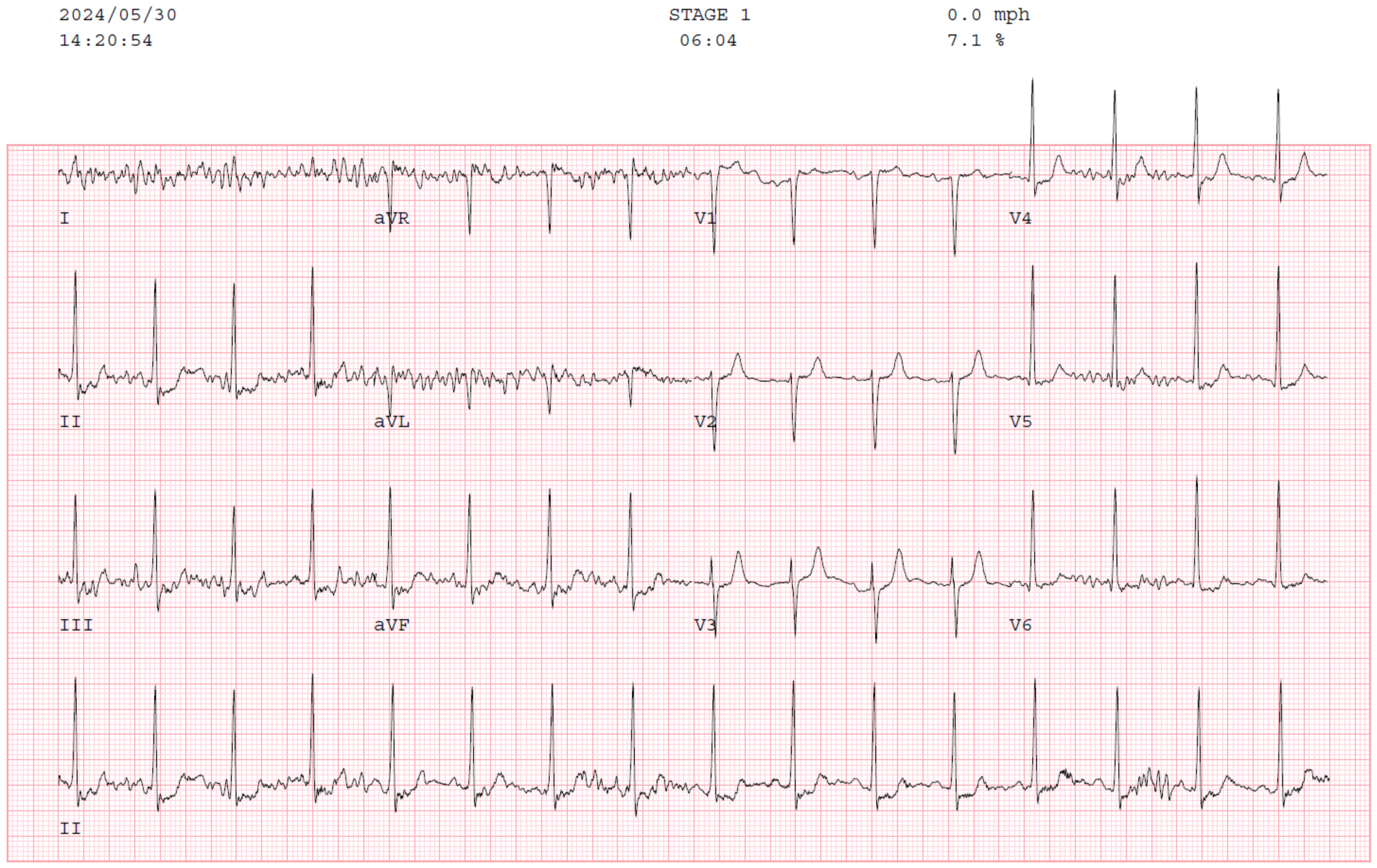
Relevant Test Results Prior to Catheterization
Echocardiography revealed focal hypokinesia of the mid-posterior wall, with a preserved overall left ventricular ejection fraction. Non-invasive tests, including a treadmill test and myocardial perfusion imaging (SPECT) were performed. The treadmill test was positive in stage 1, but it was terminated early, within the first few minutes, due to significant dyspnea. SPECT showed normal myocardial perfusion.
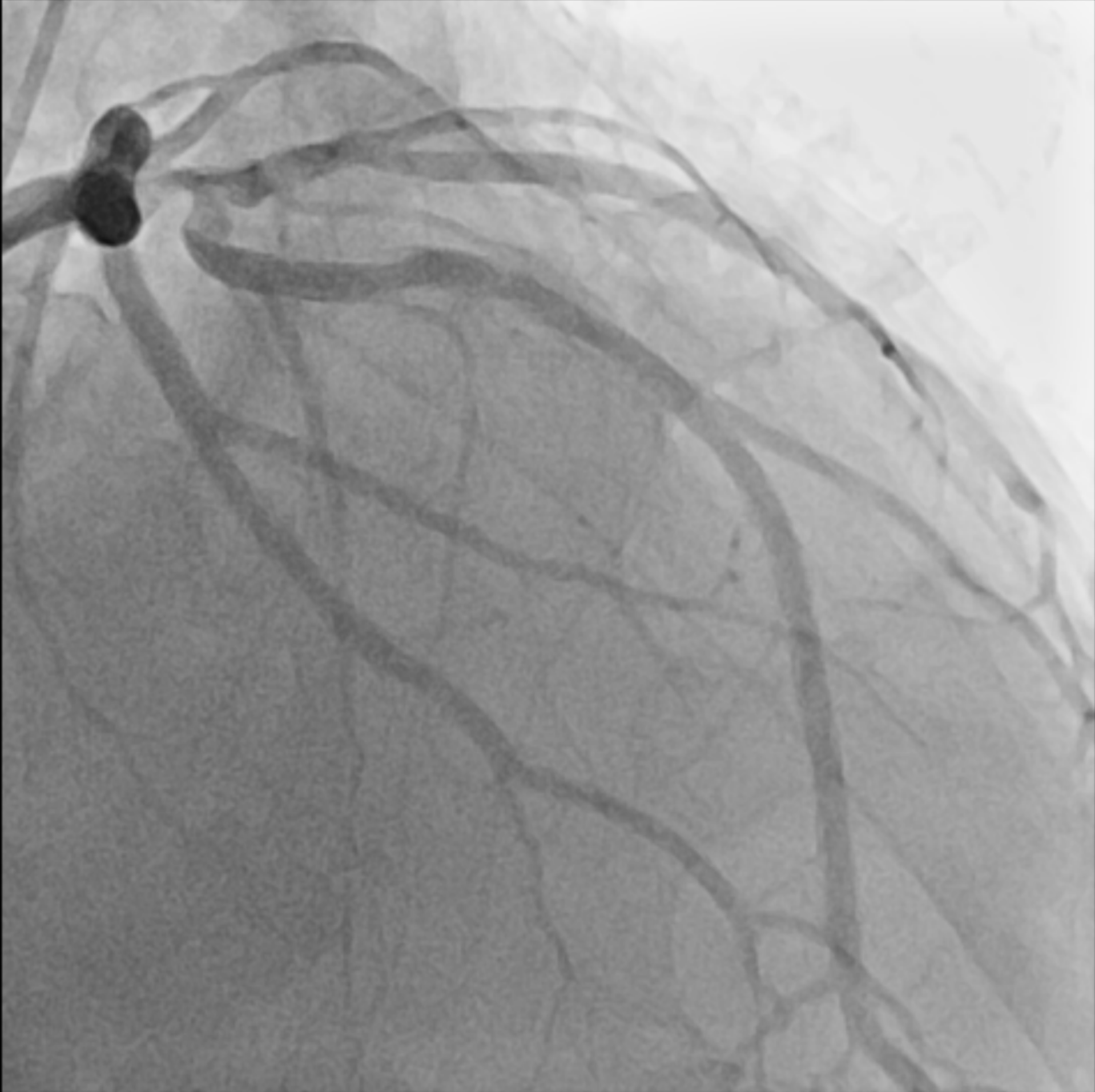
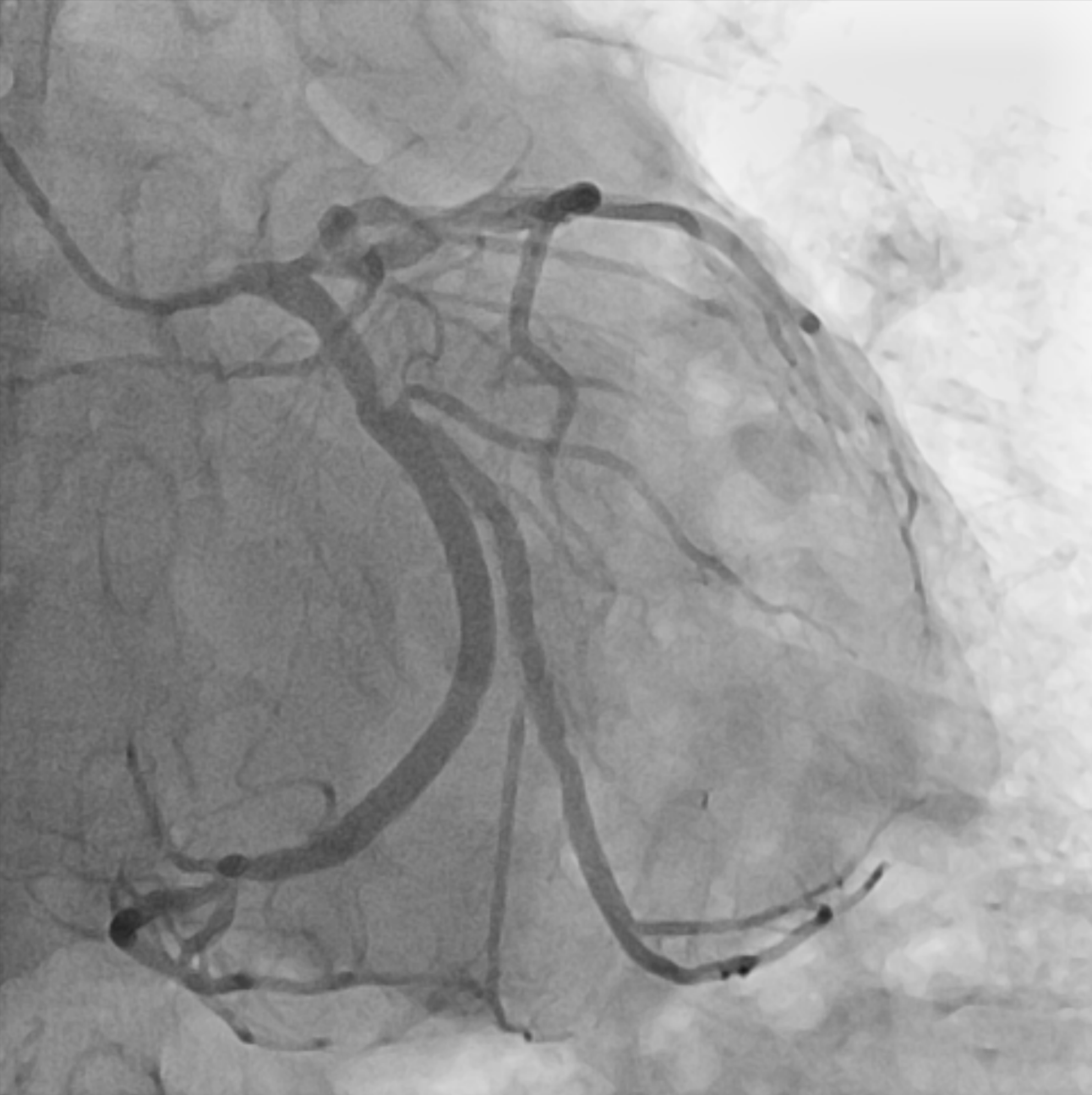
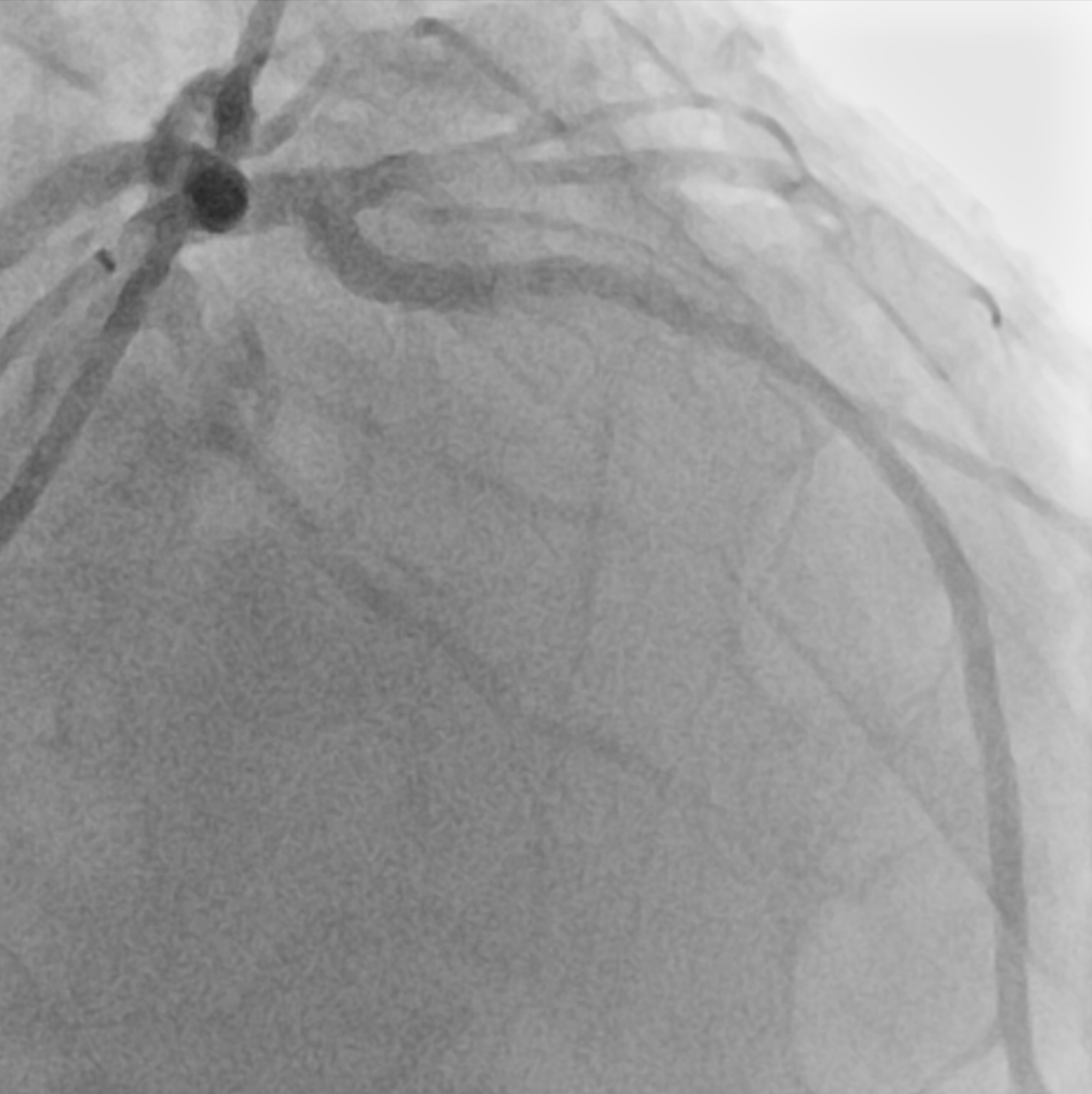
Relevant Catheterization Findings
Coronary angiography revealed a newly identified severe stenosis with tortuosity and heavy calcification in the ostium of the LAD, while the previously implanted stent in proximal LAD and OM were patent. There was no significant lesions in right coronary artery.

Interventional Management
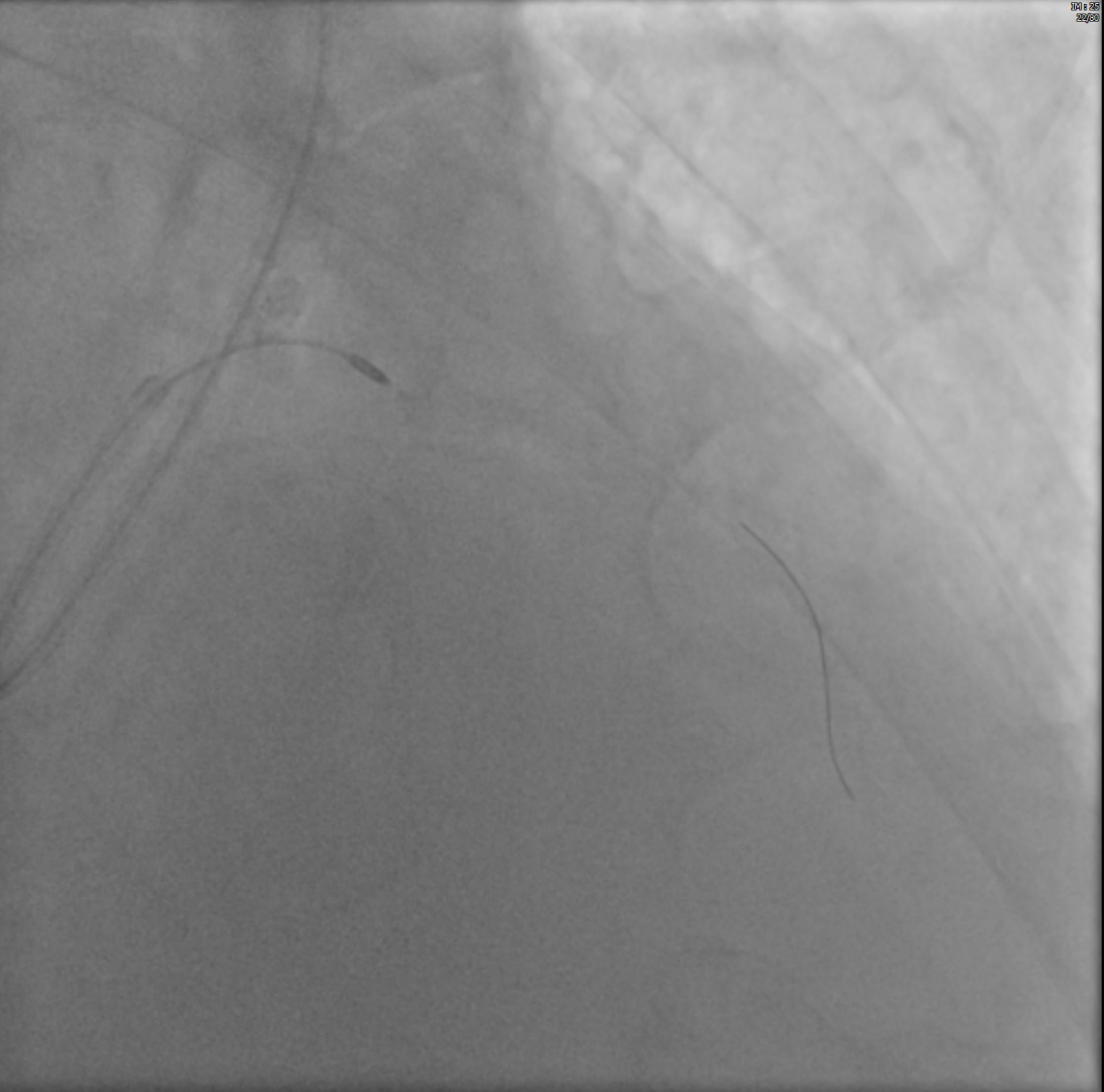
Procedural Step
The right radial artery approach was used with a left Judkins 3.5, 7Fr guiding catheter. A Sion wire successfully passed the lesions using micro-guide catheter (Caravel), followed by predilation using a Ryurei balloon 1.0 x 5 mm with 6Fr extension catheter (Guide Zilla). As a Ryurei balloon 1.5 x 15 mm failed to pass the lesion, a rotawire was used to cross the lesion, allowing for subsequent Rotablation. Rotablation with a 1.25 mm burr was performed at a speed of 145,000 to 185,000 rpm, followed by using the 1.0 x 5 mm Ryurei balloon again. Due to the persistence of heavy calcification, a second rotablation with a 1.5 mm burr at 145,000-185,000 rpm was performed, followed by the sequential use of Ryurei balloons in increasing sizes (1.0 x 5 mm, 1.5 x 15 mm, and 2.5 x 15 mm) for further lesion preparation. After using the intravascular ultrasonography (IVUS) to assess the lesion, Sapphire NC balloon 3.0 x 15 mm was used for the lesion preparation. XIENCE Skypoint stent with 3.0 x 23 mm was implanted through the lesion, followed by adjunctive ballooning with a 3.5 x 15 mm non-compliant balloon, resulting in satisfactory angiographic and IVUS outcomes.

Case Summary
Rotablation is a valuable technique in treating heavily calcified lesions, as in this case, where tortuosity and calcification created significant challenges for balloon and stent passage. For that reason, there is often hesitation in using rotablation due to the risk of procedure-related complications, such as vessel perforation, particularly in tortuous lesions. However, when performed with caution, rotablation can be both safe and effective in treating highly tortuous and heavily calcified lesions with severe stenosis, as demonstrated in this case.