CASE20240919_001
A Case of Myocardial Infarction of the Left Circumflex Artery Accompanied by Chronic Total Occlusion at Left Anterior Descending Artery with Advanced Gastric Cancer.
By Ji-Wung Ryu
Presenter
Ji-Wung Ryu
Authors
Ji-Wung Ryu1
Affiliation
Hallym University Kang-Nam Sacred Heart Hospital, Korea (Republic of)1,
View Study Report
CASE20240919_001
Complex PCI - CTO
A Case of Myocardial Infarction of the Left Circumflex Artery Accompanied by Chronic Total Occlusion at Left Anterior Descending Artery with Advanced Gastric Cancer.
Ji-Wung Ryu1
Hallym University Kang-Nam Sacred Heart Hospital, Korea (Republic of)1,
Clinical Information
Relevant Clinical History and Physical Exam
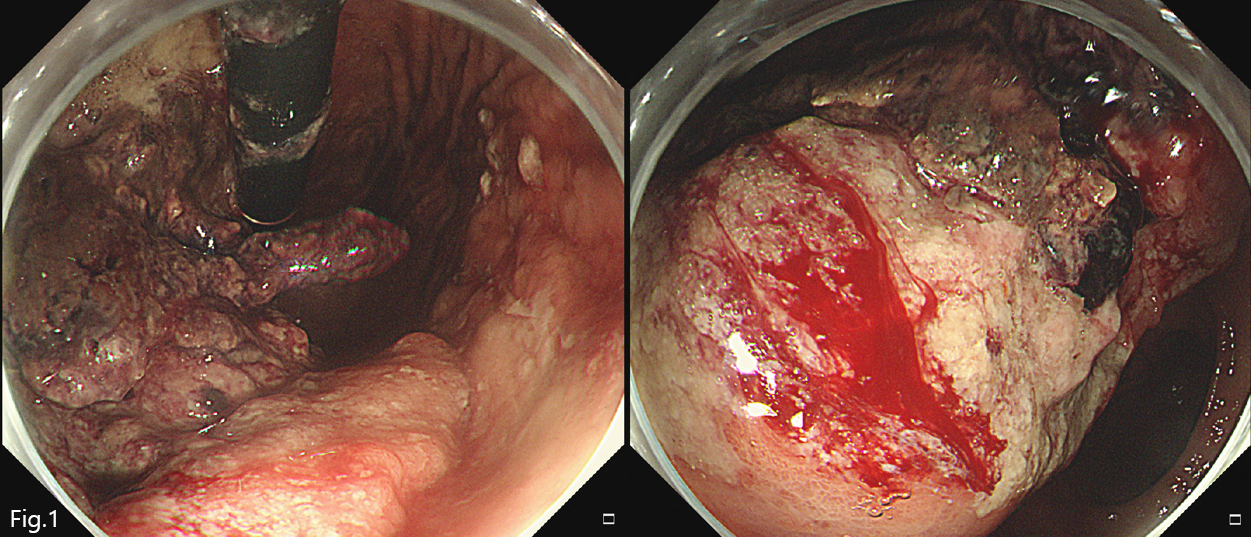
A 57-years-old male patient was consulted from general surgery for operability on advanced gastric cancer (Fig1). He had been symptom about dyspnea with orthopnea (New York Heart Association functional class II) one month ago. He had been current smoking history for 30 pack-years. And his medical history was hypertension, anemia,diabetic mellitus.
Relevant Test Results Prior to Catheterization
The transthoracic echocardiography revealed reduced left ventricular ejection fraction (EF=43%) with regional wall motion compatible with left anterior descending artery (LAD) lesion.
Relevant Catheterization Findings
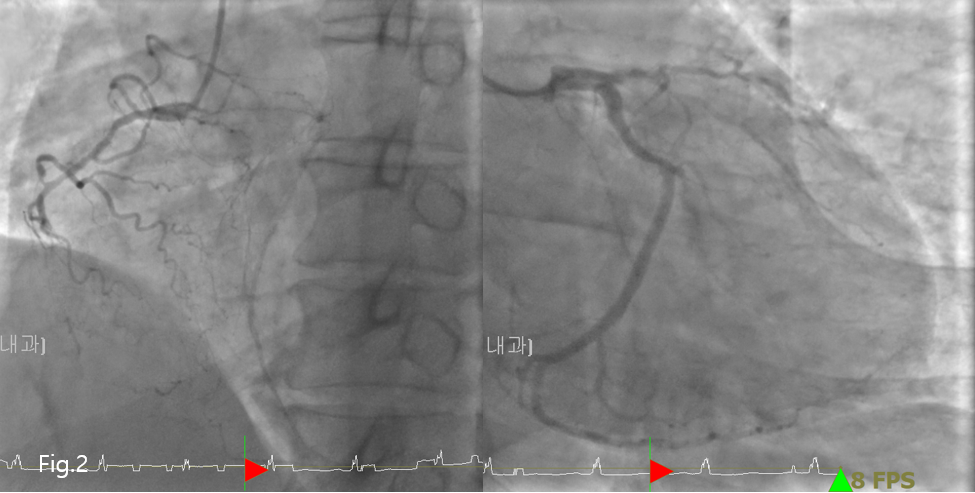
A diagnostic coronaryangiography was performed (Fig2), 3Vessel coronary artery obstructive disease(CAOD) revealed diminutive mid right coronary artery (RCA) lesion at CTO (100%,TIMI flow 0) and Big left circumflex artery (LCx) with 50% residual stenosis and vulnerable plaque and also the diffuse CTO at proximal LAD lesion. It was collateral flow from right ventricular branch to mid to distal LAD lesion withTIMI flow (grade II/III).
Interventional Management
Procedural Step
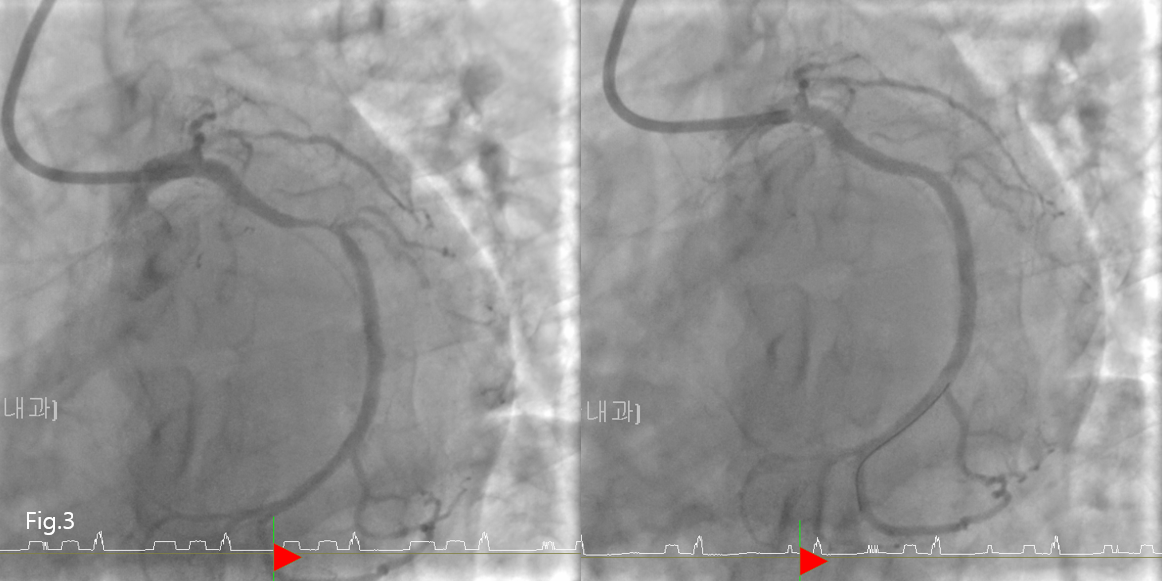
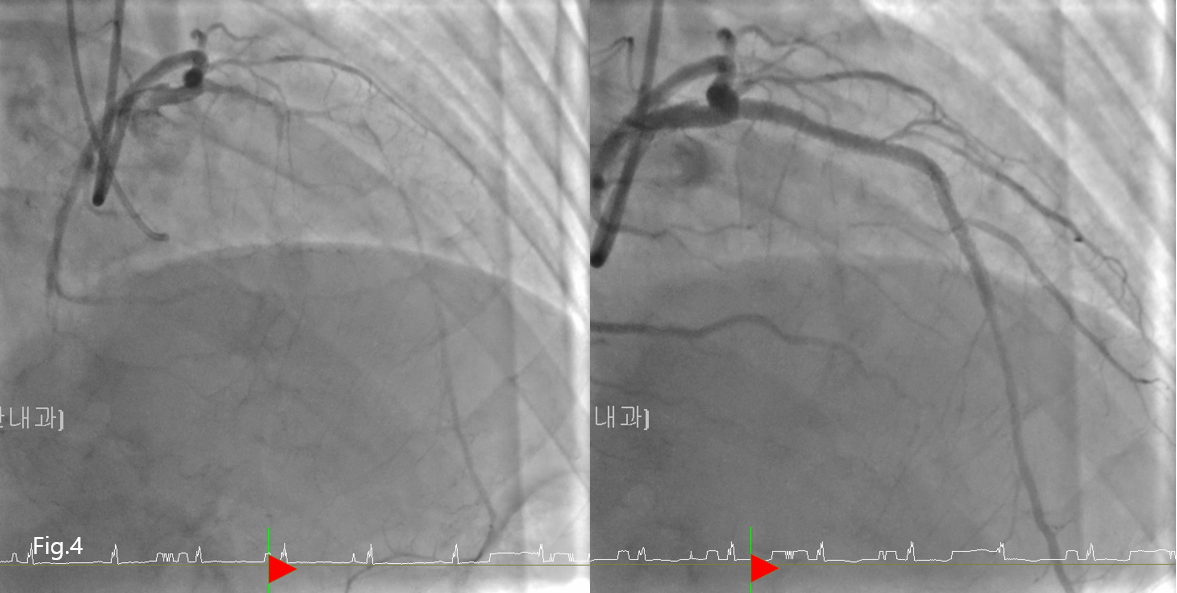
The first operation about advanced gastric cancer was done. And then, the patient had been taking a restfor 2~3 days later. He had been suddenly chest pain and blood pressure dropping. Cardiac marker was elevation. Troponin-T was 1.270 ng/ml. CK/CK-MB was1105/65.20 ratio. I decided the coronary angiography at emergency situation for suggesting about non-ST elevation myocardial infarction (NSTEMI). It revealed that near acute total occlusion at mid LCx lesion. PCI was done (Fig3). And the patient was stable. So I decided to plan the PCI about CTO at proximal LAD lesion. After 4~5 days later, the patient was maximum taking a rest for bleeding complication about operation site at abdomen lesion. And then, It prepared on bi-lateral approach left radial 6Fr sheath and femoral 7Fr sheath.Anterograde approach with used intravascular ultrasound (IVUS) was done. It used on first wiring Run-though for navigating on proximal LAD lesion and micro-catheter with Fider-XT successfully. The procedure was successful result (Fig4). Chronic total occlusion was very hard and difficult procedure however, this case was meaningful myocardial infarction accompanied by chronic total occlusion.
Case Summary
Discussion point 1. How to solve the problem about acute coronary syndrome with malignant cancer patient on high bleeding risk and 2. The point of be careful about chronic total occlusion procedure with myocardial infarction.