CASE20240818_001
A Challenging Case of Right Subclavian Artery Approach ECMO-Support High Risk PCI with Unusual Rotawire Fracture
By Chien-Po Huang
Presenter
Chien-Po Huang
Authors
Chien-Po Huang1
Affiliation
Cheng Hsin General Hospital, Taiwan1,
View Study Report
CASE20240818_001
High-Risk Intervention - High-Risk Intervention (Diagetes, Heart Failure, Renal Failure, Shock, etc)
A Challenging Case of Right Subclavian Artery Approach ECMO-Support High Risk PCI with Unusual Rotawire Fracture
Chien-Po Huang1
Cheng Hsin General Hospital, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
An 80-year-old male with history of CAD, severe PAOD , abdominal aortic aneurysm status post stenting, Type II DM and ESRD presented with severe chest pain during hemodialysis. Diagnosed with non-ST-segment elevation myocardial infarction with reduced ejection fraction (HFrEF). CAG revealed severe calcification and significant. Due to his high-risk status, he was transferred to our hospital, where he requested PCI but declined coronary artery bypass grafting.
Relevant Test Results Prior to Catheterization
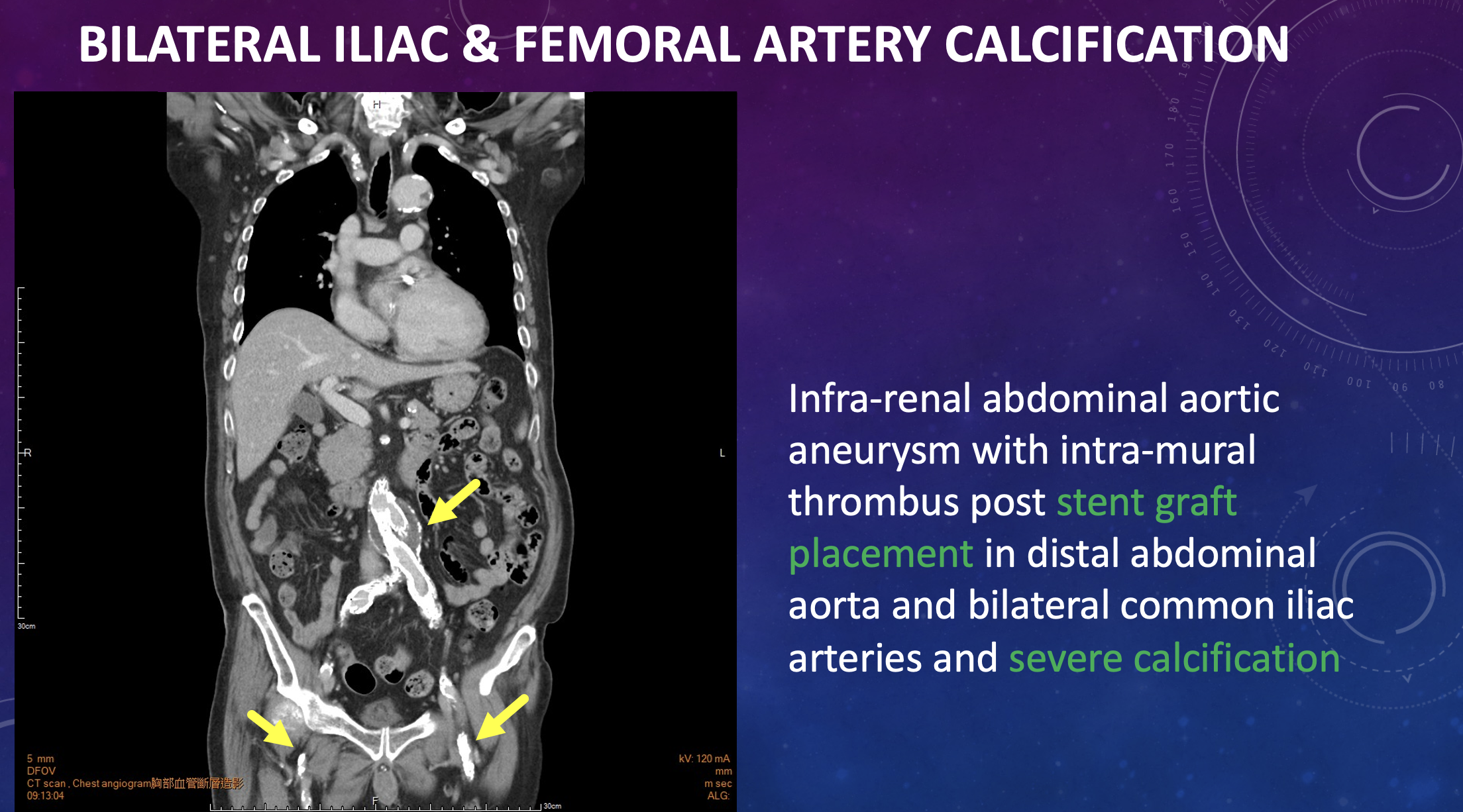
Lab results showed Troponin-I at 1593 pg/mL, CK-MB at 12 ng/mL, and creatinine at 7.03 mg/dL. TTE revealed LVEF of 28%, generalized hypokinesia, akinesia of the basal inferior and basal middle posterior walls, and severe mitral regurgitation (MR) with Carpentier types I and IIIb. A whole-body CT angiogram indicated bilateral iliac and femoral artery calcification and an infra-renal abdominal aortic aneurysm with with intra-mural thrombus post stent graft placement.
Relevant Catheterization Findings
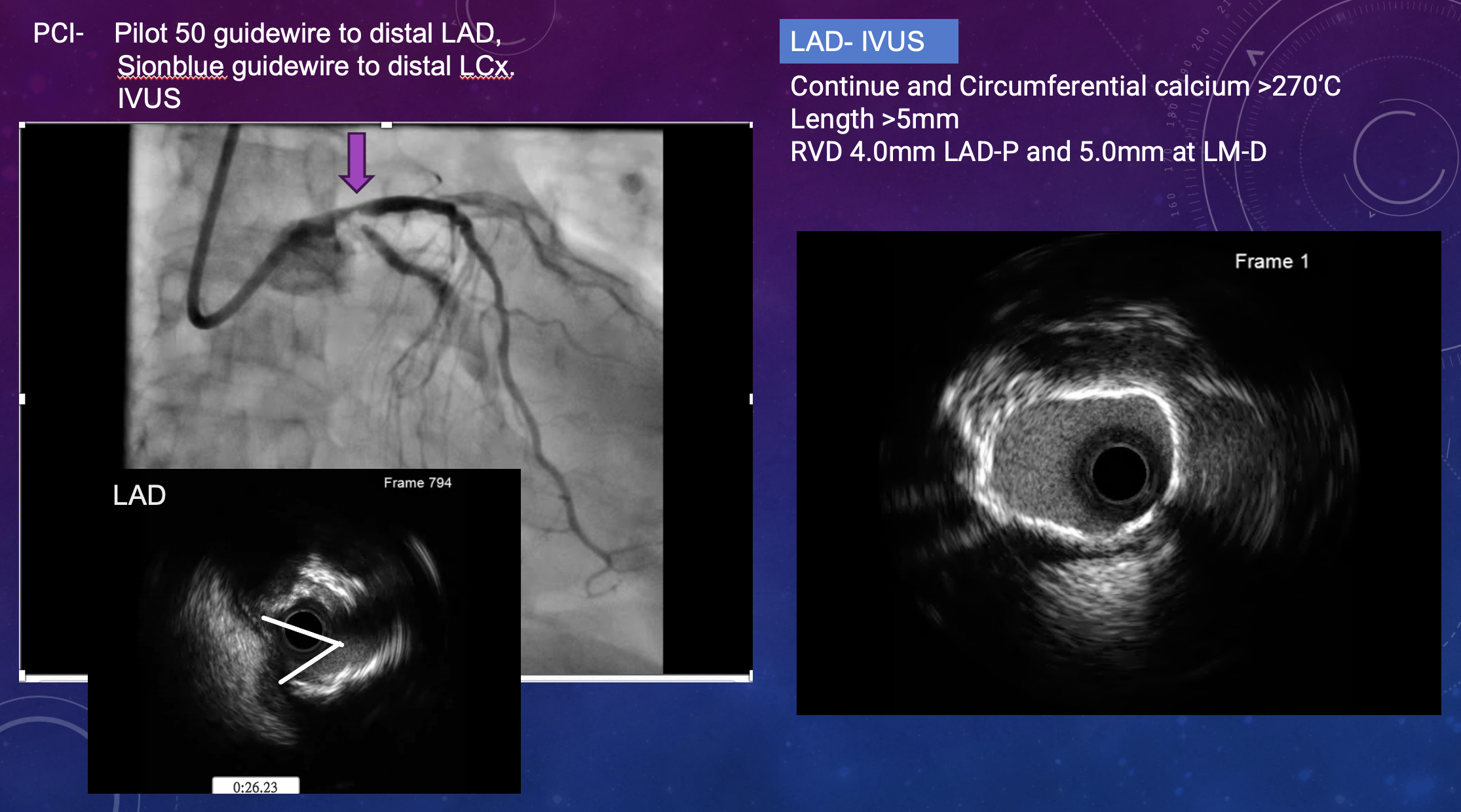
Coronary angiogram findings included heavy calcification with a calcium nodule and thrombus causing 95% stenosis in the left circumflex artery (LCx), as well as severe calcification and 80-90% stenosis in the left anterior descending artery (LAD). The RCA showed chronic total occlusion (CTO) of the RCA-P. ECMO-supported PCI using RotaTripsy was suggested after a heart team discussion.


Interventional Management
Procedural Step
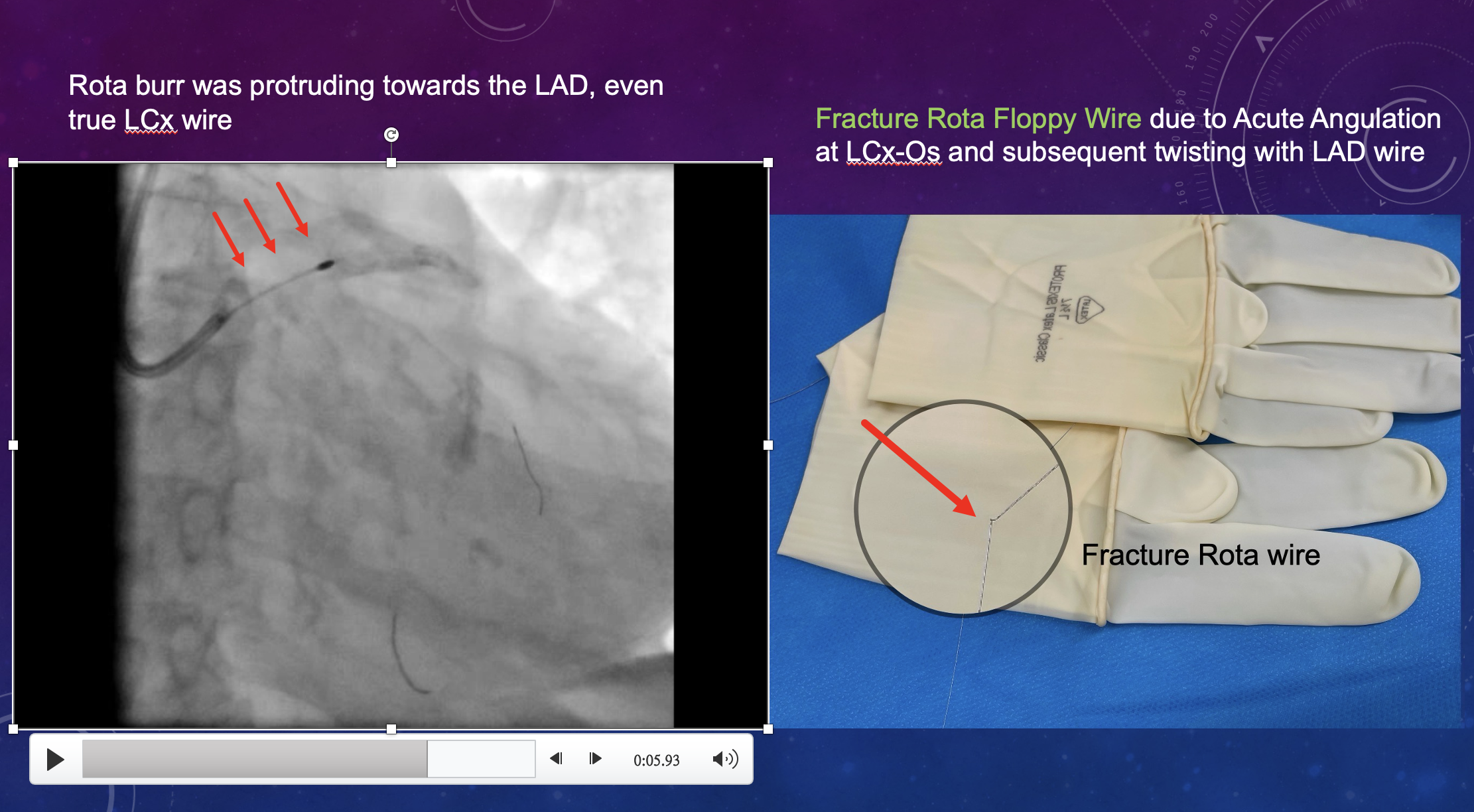
Guidewires were advanced to the distal LAD and LCx, followed by intravascular ultrasound (IVUS) revealing severe circumferential calcification. Rotational atherectomy was performed, but complications arose, including a fractured Rota floppy wire due to acute angulation at the LCx-ostium. After carefully exchanging the wire, intravascular lithotripsy (IVL) was attempted but initially failed to cross the LCx-ostium lesion. Sequential balloon dilatation was then performed, followed by successful IVL to the LCx-P using the balloon anchor technique. The procedure continued with stent deployment and post-dilatation, achieving relative stent expansion and apposition without edge dissection or tissue protrusion.
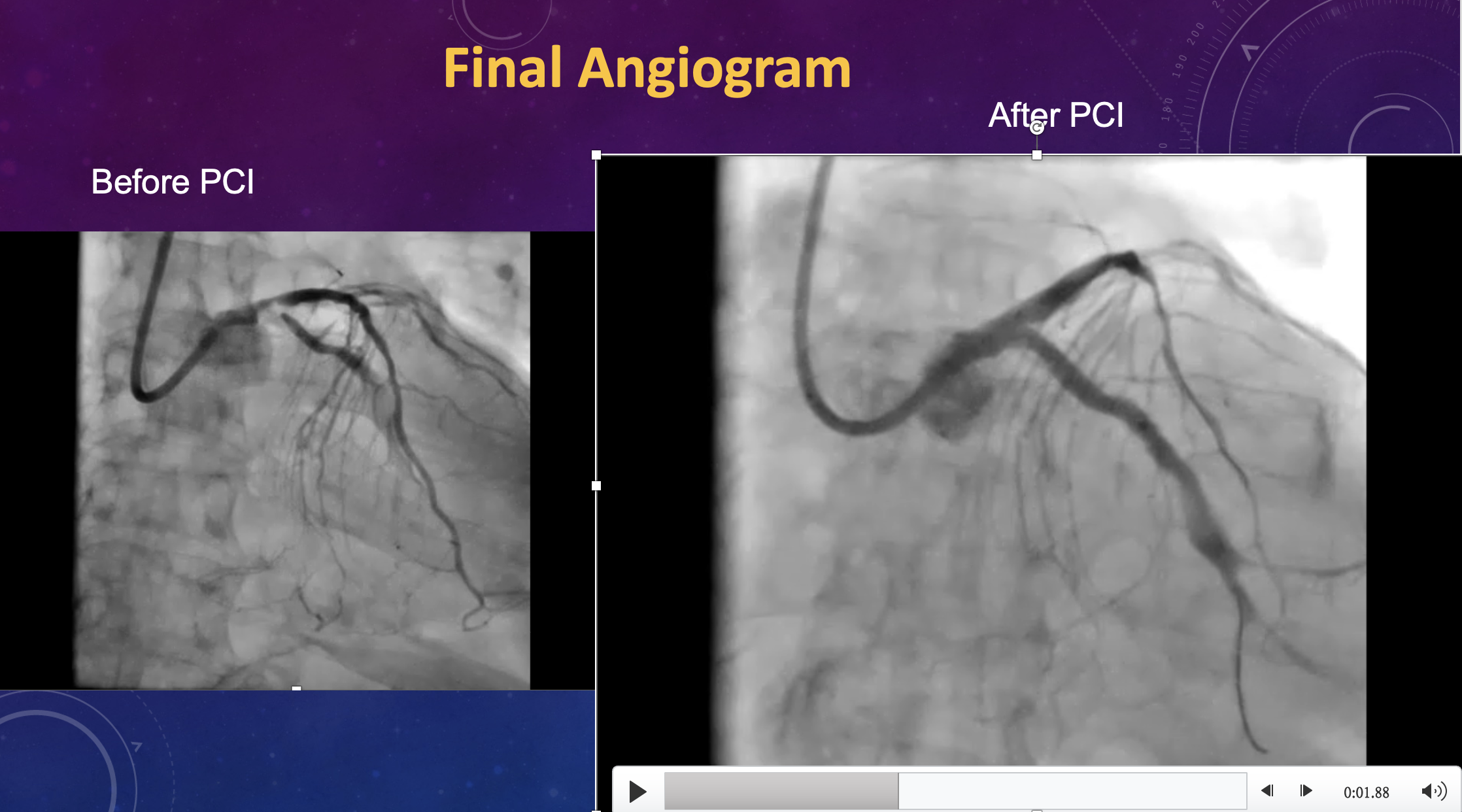
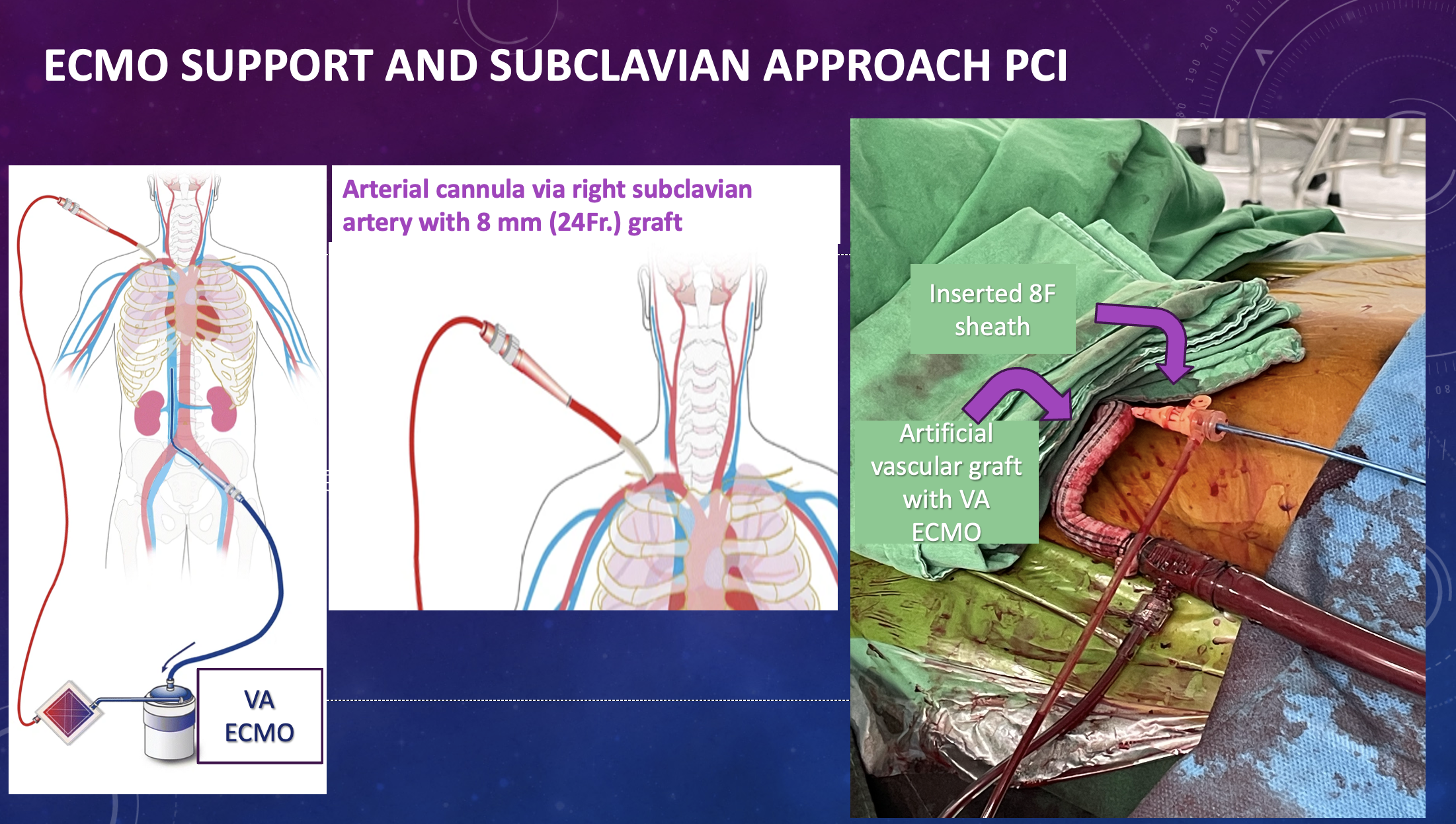
Case Summary
RotaTripsy was performed in a heavily calcified left main coronary bifurcation stenosis under VA-ECMO support, with an arterial cannula inserted via the right subclavian artery approach. This method was chosen due to the patient’s severe peripheral vascular disease in the lower limbs, which made conventional femoral artery and vein cannulation less feasible. The alternative technique was selected to overcome the challenges posed by the extensive calcification in the iliac and femoral arteries.