CASE20240817_002
Early Restenosis of Inadequately Debulked Calcified Lesion
By Hao Neng Fu, Jing Ling, Chia-Hao Hung
Presenter
Chia-Hao Hung
Authors
Hao Neng Fu1, Jing Ling1, Chia-Hao Hung1
Affiliation
Cheng Hsin General Hospital, Taiwan1,
View Study Report
CASE20240817_002
Complex PCI - Calcified Lesion
Early Restenosis of Inadequately Debulked Calcified Lesion
Hao Neng Fu1, Jing Ling1, Chia-Hao Hung1
Cheng Hsin General Hospital, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
A 66-year-old man with underlying history of CAD, hypertension and hyperlipidemia, presented for angina pectoris. His coronary intervention history included PCI and stenting to LAD & RCA in 2010, to LAD-DB in 2016 and to mid LAD in 2019. First coronary angiogram was done in October, 2023 which illustrated critical stenosis in mid & distal RCA. IVL, PCI and stenting was done. But within < 10 months duration, he presented with ACS and CAG showed critical restenosis.
 RCA lesion_1st time_Pre PCI.AVI
RCA lesion_1st time_Pre PCI.AVI
RCA_1st time_Post PCI.AVI
RCA_2nd time_Pre PCI.AVI
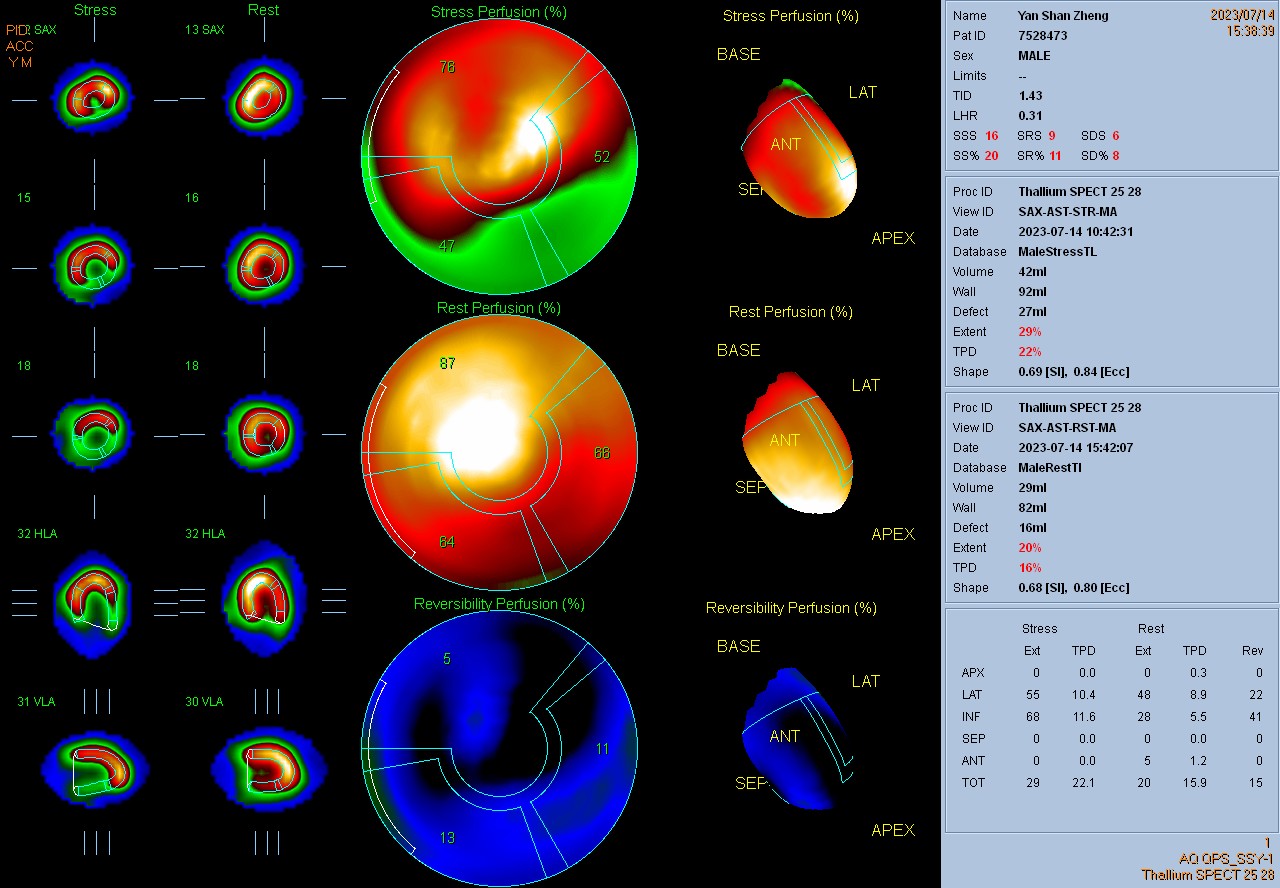
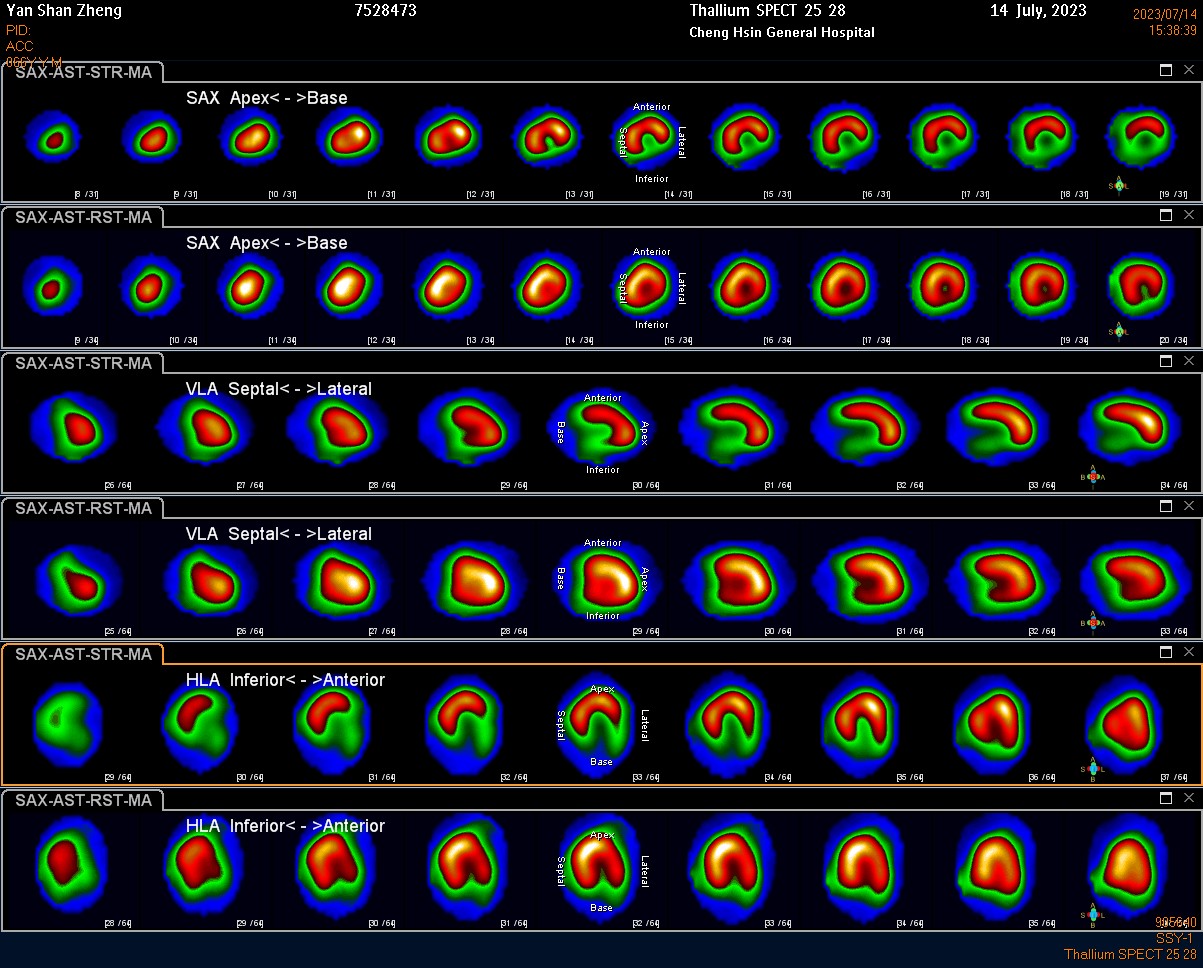
Relevant Test Results Prior to Catheterization
Stress myocardial perfusion scan illustrated inducible perfusion defect in RCA territory.
Relevant Catheterization Findings
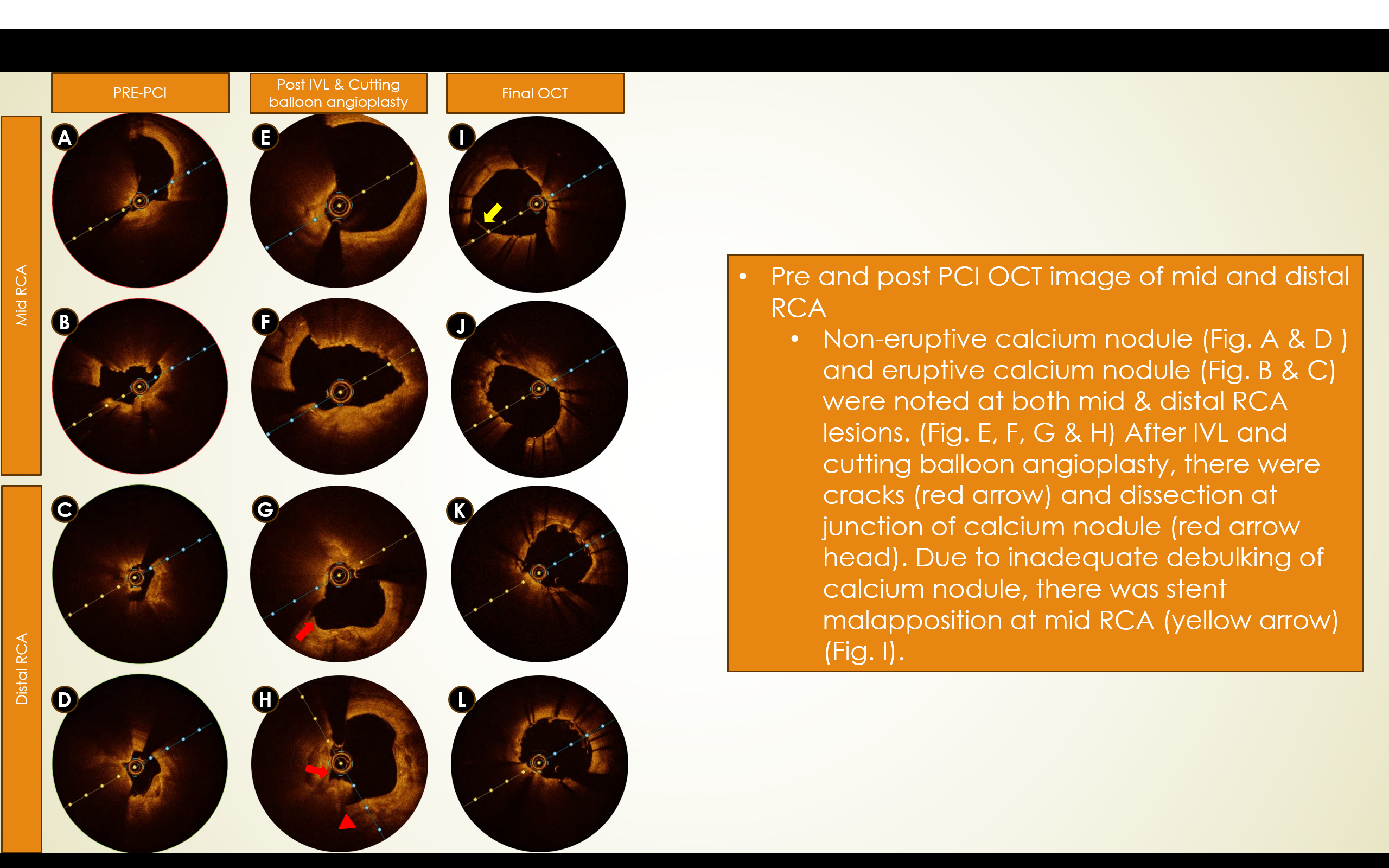
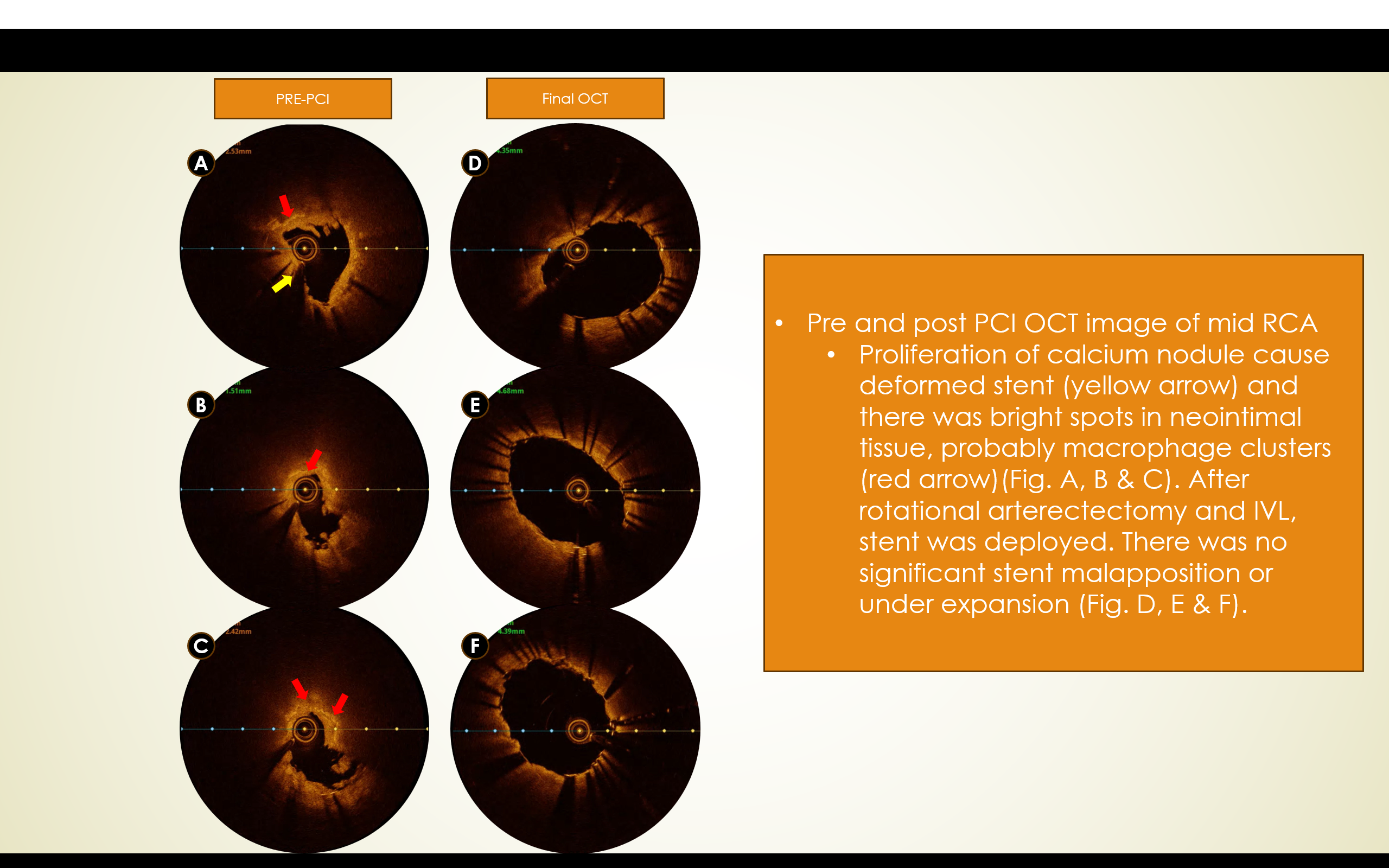
First CAG was done in October, 2023 which illustrated ciritcal stenosis in mid and distal RCA. IVL and PCI with DES stenting was done. OCT was done which illustrated eruptive & non-eruptive calcium nodules. But withitn < 10 months duration, he presented back to EMR with ACS. CAG revealed critical stenosis at mid RCA with compromised flow. OCT illustrated deformed stent and severe neointimal hyperplasia with macrophage deposition. Rotational arterectomy, IVL and PCI with stenting were done.
Interventional Management
Procedural Step
During 1st OCT guided PCI session, IVL with 3.5mm Shockwave balloon (40 pulses each for both lesions) and cutting balloon angioplasty (with 3.0mm Wolverine balloon) were done to mid and distal RCA lesions. DESs were deployed after that. Final OCT of mid RCA showed stent malapposition as calcium nodule was inadequatedly debulked. During 2nd OCT guided PCI session (approximately 7 months later), rotational artherectomy (with 2.0mm & 2.25mm Rota burr) was done to ablate overlying stent struts, and then, IVL was done with 4.0mm Shockwave balloon (all 80 pulses at mid RCA). DES was deployed after that. As calcium was adequately debulked & softened, it could deform with stent and OCT illustrated optimal stent apposition and expansion.
RCA_2nd time_Post PCI.AVI
Rotablation.AVI
IVL.AVI
Case Summary
Eruptive CN had worse outcome after PCI compared to non-eruptive CN. Adequate calcium modification (with atherectomy and/or lithotripsy) required before stenting. Inadequate calcium modification/debulking may lead to early in-stent restenosis. Intravascular imaging guided PCI is mandatory in coronary intervention for calcified coronary lesion.