CASE20240816_010
A Case of ECMO Supported PCI in a Patient with Severe Aortic Stenosis and End Stage Renal Failure
By Ka Lung Chui
Presenter
Ka Lung Chui
Authors
Ka Lung Chui1
Affiliation
Prince of Wales Hospital, Hong Kong, China1,
View Study Report
CASE20240816_010
High-Risk Intervention - High-Risk Intervention (Diagetes, Heart Failure, Renal Failure, Shock, etc)
A Case of ECMO Supported PCI in a Patient with Severe Aortic Stenosis and End Stage Renal Failure
Ka Lung Chui1
Prince of Wales Hospital, Hong Kong, China1,
Clinical Information
Relevant Clinical History and Physical Exam
Male, 63 year old, known HT, hyperlipidemia, CVA, ESRF on CAPDAdmitted for loss of consciousness and chest painECG on admission showed anterior and inferior Q wave, AVL and lead I ST depressionHigh sensitive TNT >50000CVS grade 3/6 ejection systolic murmur radiate to both carotid arteriesEcho confirmed severe AS, moderate AR, EF 25% onlyCoro showed LAD calcified LAD CTO, dLCx occluded, RCA minor disease, PLB severe stenosis but smallPre-TAVI was performed
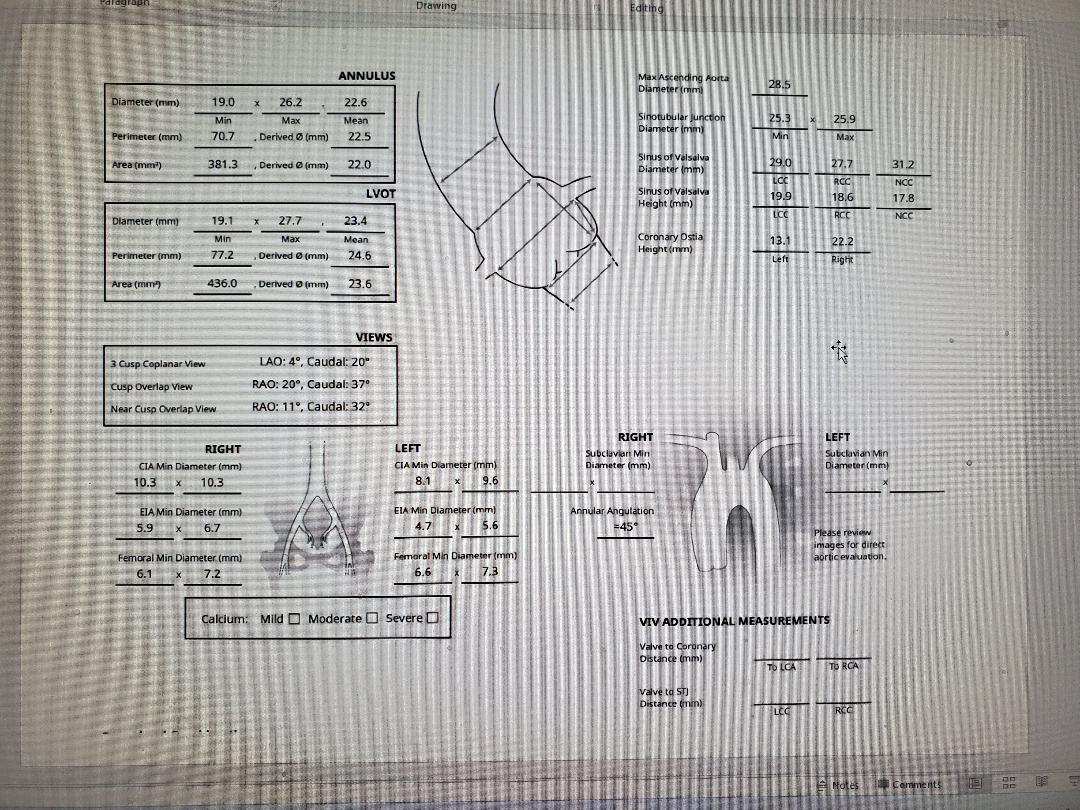
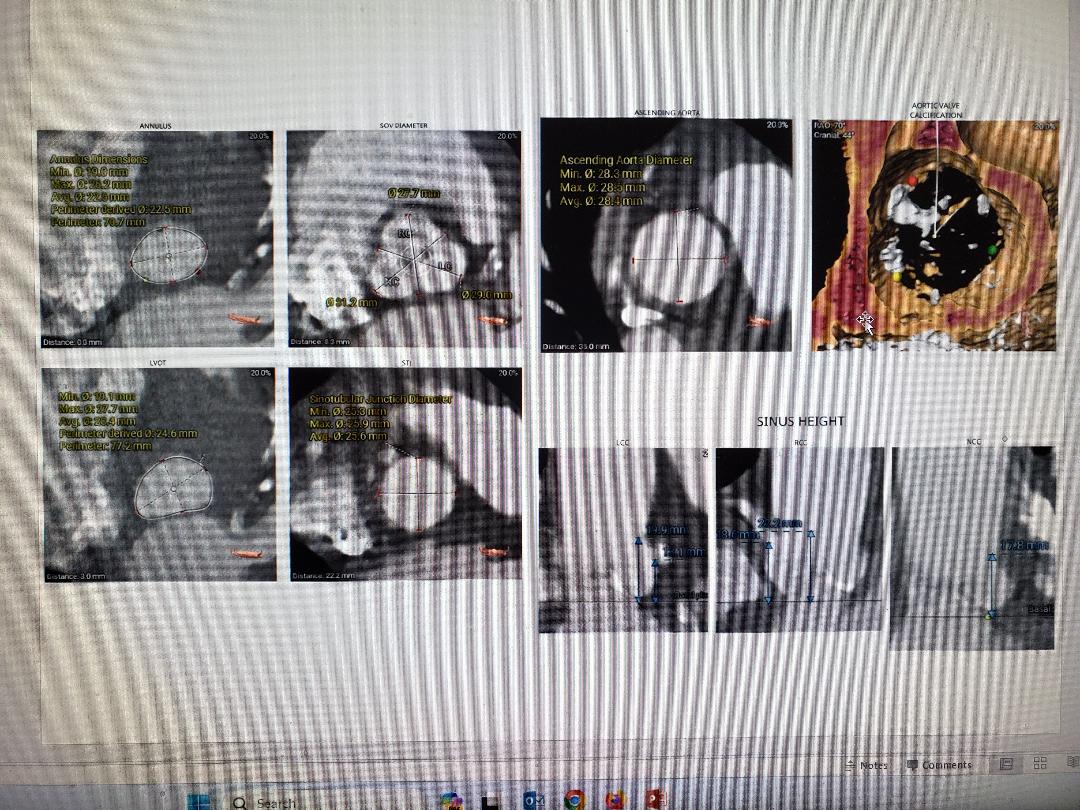
 pre tavi CT.jpeg
pre tavi CT.jpeg
Relevant Test Results Prior to Catheterization
Echo showed severe impaired LV systolic function, LVEF 25%, heavily calcified aortic valve with severe low flow low gradient AS and moderate ARAVA = 0.52cm2
Relevant Catheterization Findings
Coronary angiogram showed heavily calcified vessels, LM normal, mLAD subtotal occlusion followed by total occlusion, dLCx occluded, RCA minor disease, PLB severe stenosis but small.
Interventional Management
Procedural Step
ECMO was inserted for hemodynamic supported before the procedure, TAVI was performed first using accurate neo 2 size M valve, as there was moderate AR and this valve did not hinder the coronary access in this case. After the valve was deployed, PCI was performed using EBU 3.5 guide, fielder XTA crossed the CTO but nothing crossed as lesion is too calcified. Primary wiring with rotadrive wire into distal LAD, rota 1.25mm burr for few passes, followed by shockwave 2.5mm balloon and NC balloon. Decided for DCB at the end due to satisfactory angiographic result.
Case Summary
This patient was in cardiogenic shock requiring pressor, poor EF 25% only, he is at high risk of complications if PCI was performed before the TAVI. His LVEF further deteriorated while waiting for pre-TAVI CT with 1 episode of PEA arrest. Hemodynamic supported during the procedure is neccessary. We chose ECMO as this can be used to support both TAVI and PCI procedure. With ECMO support, procedure went smoothly and patient was discharged home afterwards. (i have done this case yesterday and i don't have the time to download the cine, will upload it to you later on)