CASE20240816_006
No Cross, No Crown
By Po-Chih Lin
Presenter
Po-Chih Lin
Authors
Po-Chih Lin1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
CASE20240816_006
Complex PCI - CTO
No Cross, No Crown
Po-Chih Lin1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
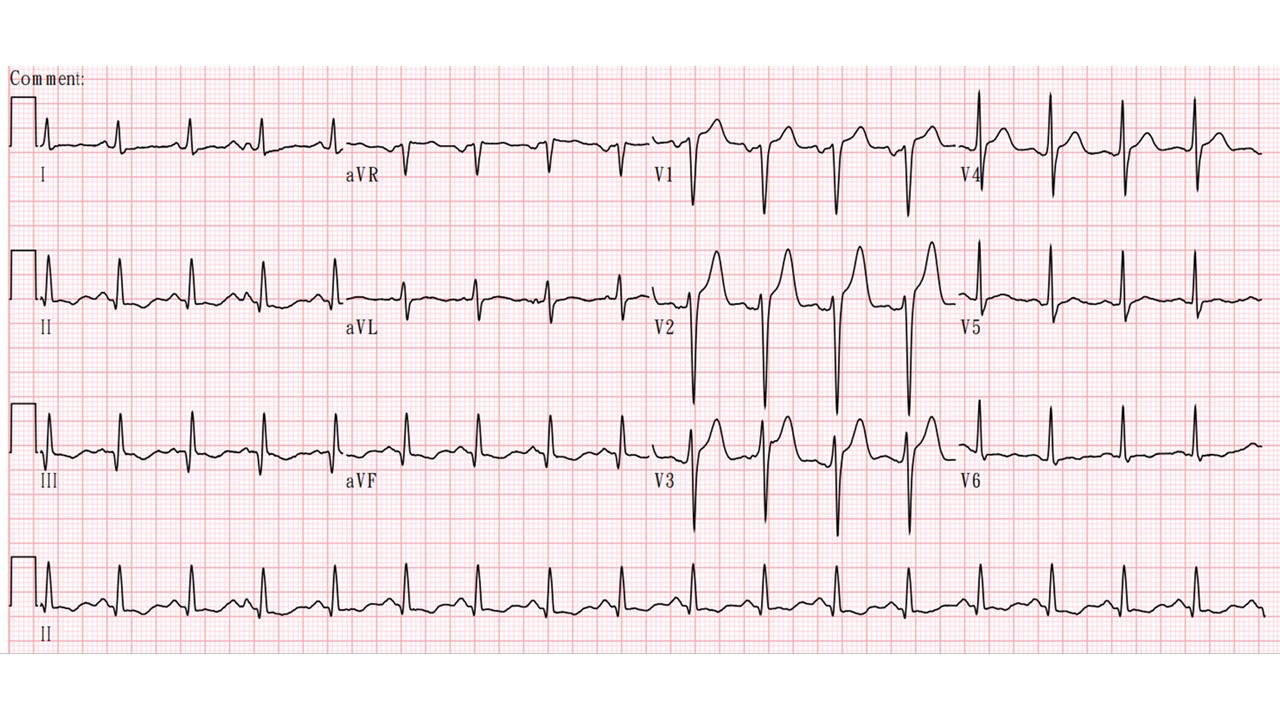
A 48-years-old man had a witness collapse in a barbor shop, with bystander CPCR and AED shock 3 times with ROSC when EMT arrived. He had past history of HTN, hyperlipidemia, CAD, 3VD status post RCA stenting 8 years ago. Anterior STEMI was noted so primary PCI was activated. The culprit is middle LAD 99% stenosis which was stented directedly. He also had non-dominant distal LCX total occlusion and proximal RCA CTO, collateral from LAD. The patient received RCA CTO PCI in the next admission.
 1st PPCI mLAD.wmv
1st PPCI mLAD.wmv
1st PCI RCA.wmv
Relevant Test Results Prior to Catheterization
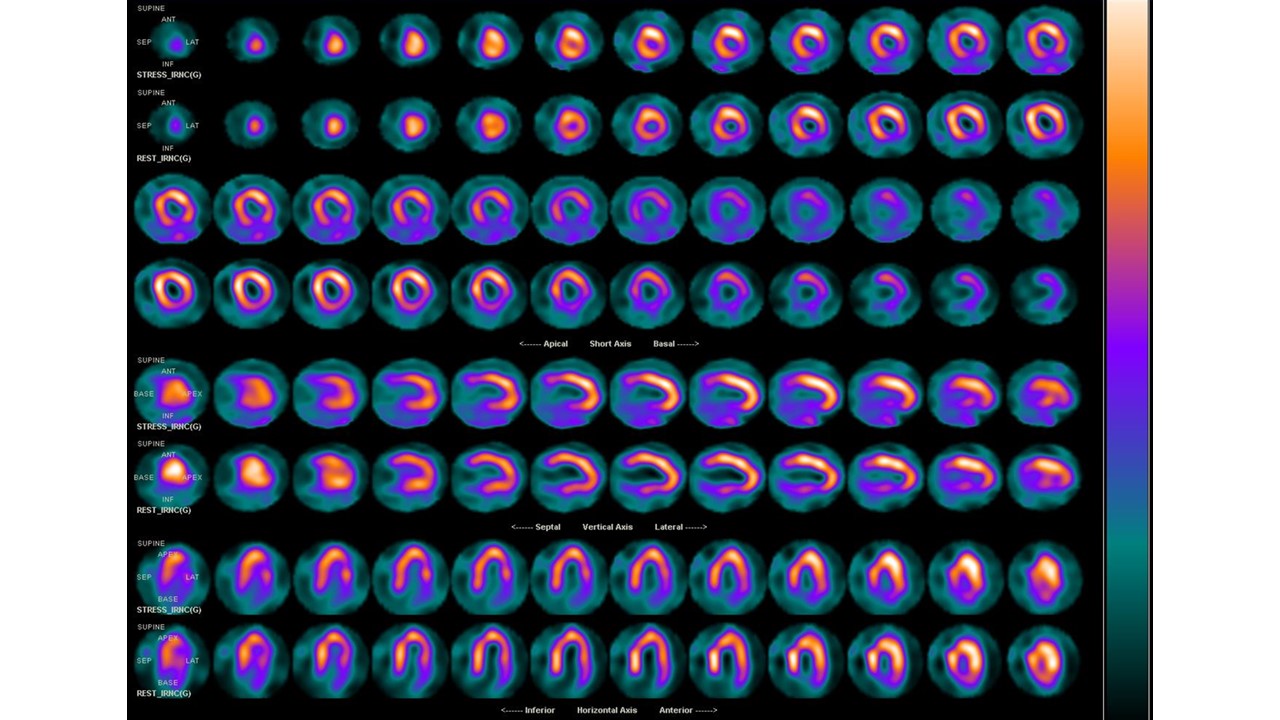
Due to the patient still has CCS class II angina, he received Dipyridamole stress Thallium-201 scan two months later. Inferior reversible perfusion defects were noted. Thus, he was admitted for RCA ISR CTO PCI.
Relevant Catheterization Findings
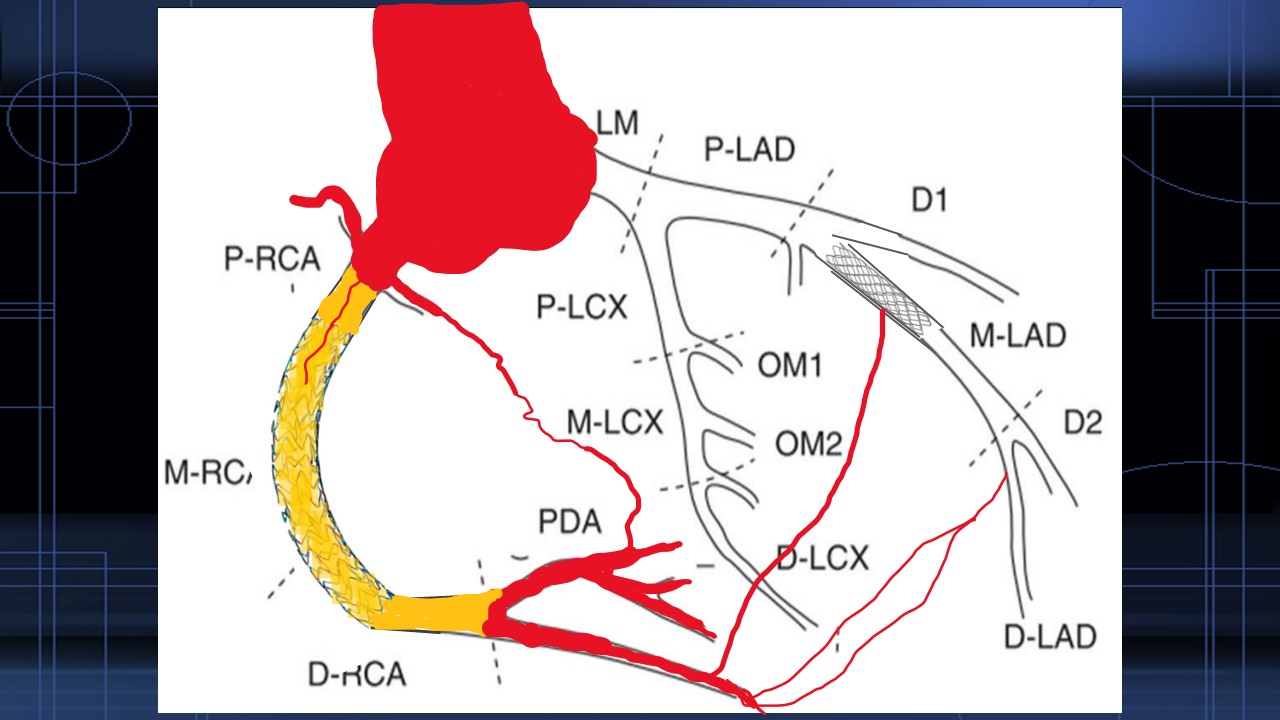
Coronary angiograpghy during this admission revealed previous mLAD stent maybe undersize. Distal LCX and OM branch was CTO with ipisilateral LAD collateral. Proximal RCA ISR totally occluded with LAD collateral from several septal branch.
LCA2.wmv
RCA2.wmv
Contralateral injection.wmv
Interventional Management
Procedural Step
I chose right femoral 7Fr SAL guilding forantegrade approach first, LRA glidesheath 7Fr EBU 3.5 to LCA for contralateralinjection. Antegrade wiring from Fielder XTA, Ultimate bro3, Gaia first to Conquest pro but failed topuncture through proximal CTO cap. I shifted to retrograde approach.I chose SION Blue with Corsairmicrocatheter from septal branch collateral between LAD stent strut. Failedretrograde wire reach distal RCA bifurcation, and I switched to conquest profor retrograde CTO cap puncture, wire into subintimal, making some hematoma.I shifted back toantegrade approach and GC was switched to 7Fr AL1, GW escalated to Conquest pro820. After proximal CTO cap puncture through, wire switched to Gaia 3rd andpass ISR CTO.I switched both antegrade and retrograde wire into fielder FC, made kissing wire. Finally antegrade using SION Blue into distal true lumen. I performed reverse CART and insert 2nd Fielder FC wire into PDA. IVUS confirmed in true lumen and I performed stenting from pRCA to PLA/PDA bifurcation. mLAD stent was dilated with NC 3.0 but no flow was noted, favor distal stent edge dissection. One stetn was placed from distal stent edge and final LAD is good.
retrograde Conquest pro failed passing dRCA.wmv
Case Summary
Thi This is the longest CTO procedure time in my clinical practice in 2023. Total fluoroscopy time 198 minutes, air Kerma 9397mGy, procedure tiem 6.5hrs and contrast using 260mL. Luckily patient had no radiation side effects. There are a lot of flaw during my procedure and may have some learning points could be discussed. It would be my honor if I have a chance to present this case in COMPLEX PCI 2024.