CASE20240816_003
A Case of LMT-LAD/LCX Medina Type 1.1.1 Bifurcation Lesion Treated with DCA
By Yuma Yamakawa
Presenter
Yuma Yamakawa
Authors
Yuma Yamakawa1
Affiliation
Shuuwa General Hospital, Japan1,
View Study Report
CASE20240816_003
Complex PCI - Left Main
A Case of LMT-LAD/LCX Medina Type 1.1.1 Bifurcation Lesion Treated with DCA
Yuma Yamakawa1
Shuuwa General Hospital, Japan1,
Clinical Information
Relevant Clinical History and Physical Exam
A 62-year-old man presented to our hospital with exertional chest pain that had been present for one month. The patient had a history of ureteral stones and a herniated disc. No risk factors for atherosclerosis such as hypertension, diabetes, dyslipidemia or smoking history were found. On examination, there were no symptoms of heart failure or other abnormalities of note.
Relevant Test Results Prior to Catheterization
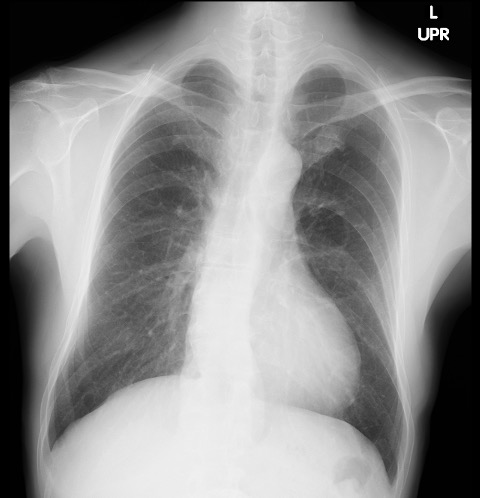
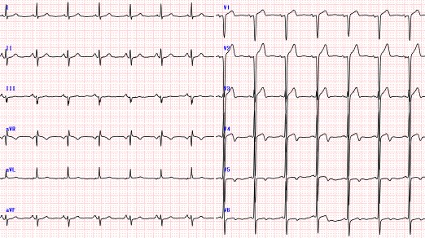
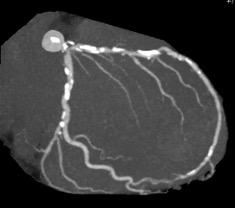
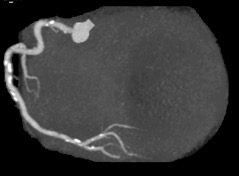
Elevated myocardial deviation enzymes and electrocardiographic changes were not observed, but echocardiography showed mild hypokinesis of mid-apex anterior LV wall. A coronary CT scan revealed severe stenosis from the left main coronary artery (LMT) to the anterior descending branch (LAD) and the circumflex branch (LCX).
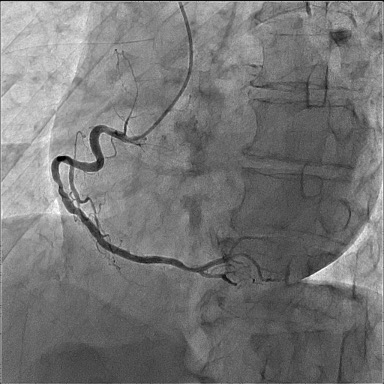
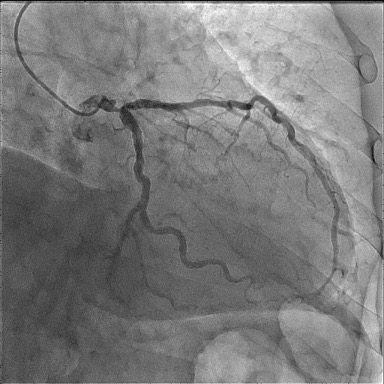
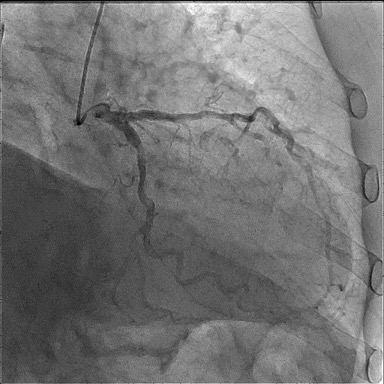
Relevant Catheterization Findings
Coronary angiography showed right coronary artery #2 50%, #3 75% stenosis and medina classification (1,1,1) lesion with 90% stenosis from LMT to LAD/LCX.
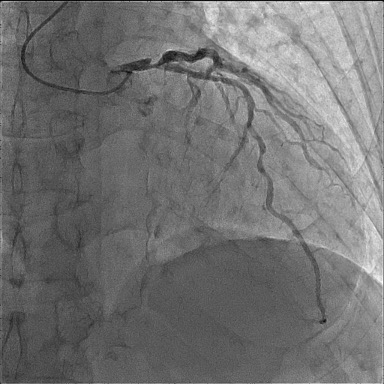
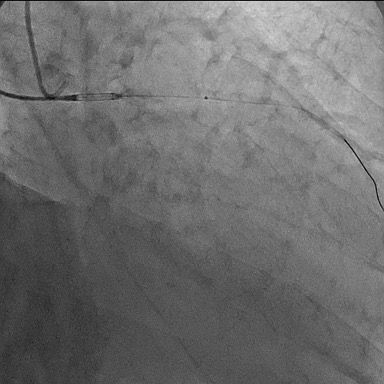
Interventional Management
Procedural Step
We changed 4Fr sheath in right radial artery to 7Fr sheath, and 4Fr sheath was placed from the right brachial artery. The IABP was placed from the right femoral artery. 7Fr CL4.0 was used for engage and 4Fr JL4.0 was placed from the 4Fr sheath for contrast confirmation. After wiring with SION blue, we changed the wire to DCA (Directional Coronary Atherectomy) wire (ABYS) using micro catheter (Mogul) and confirmed the positional relationship with the wire by IVUS and DCA was performed from 0 to 2 atmospheres. Plaque reduction was good, and the plan was to perform DCA on the LMT-LAD side. After changing the wire to ABYS again and confirming the position of the wire with IVUS, DCA was performed from 2 to 4 atmospheres. Plaque reduction was good, and POBA was performed on LADos and LCXos with Wolverine 4.0*10mm. Finally, KBT with 2 DCBs (SeQuent Please NEO 4.0*20mm, SeQuent Please NEO 4.0*25mm) was performed over LMT-LAD/LCX to obtain good dilation and the procedure was completed.

Case Summary
This patient had a multivessel lesion involving the left main coronary artery and could have undergone coronary artery bypass surgery, but DCA was useful in terms of perfoming stentless PCI with good plaque reduction.