CASE20240816_002
A Challenging Case of Retrograde Approach of RCA and LCx CTO
By Song Weng Ryan Khoo, Dautov Rustem, Houng Bang Liew, Wei Loong Chong
Presenter
Song Weng Ryan Khoo
Authors
Song Weng Ryan Khoo1, Dautov Rustem2, Houng Bang Liew1, Wei Loong Chong1
Affiliation
Queen Elizabeth II Hospital, Malaysia1, The Prince Charles Hospital, Australia2,
View Study Report
CASE20240816_002
Complex PCI - CTO
A Challenging Case of Retrograde Approach of RCA and LCx CTO
Song Weng Ryan Khoo1, Dautov Rustem2, Houng Bang Liew1, Wei Loong Chong1
Queen Elizabeth II Hospital, Malaysia1, The Prince Charles Hospital, Australia2,
Clinical Information
Relevant Clinical History and Physical Exam
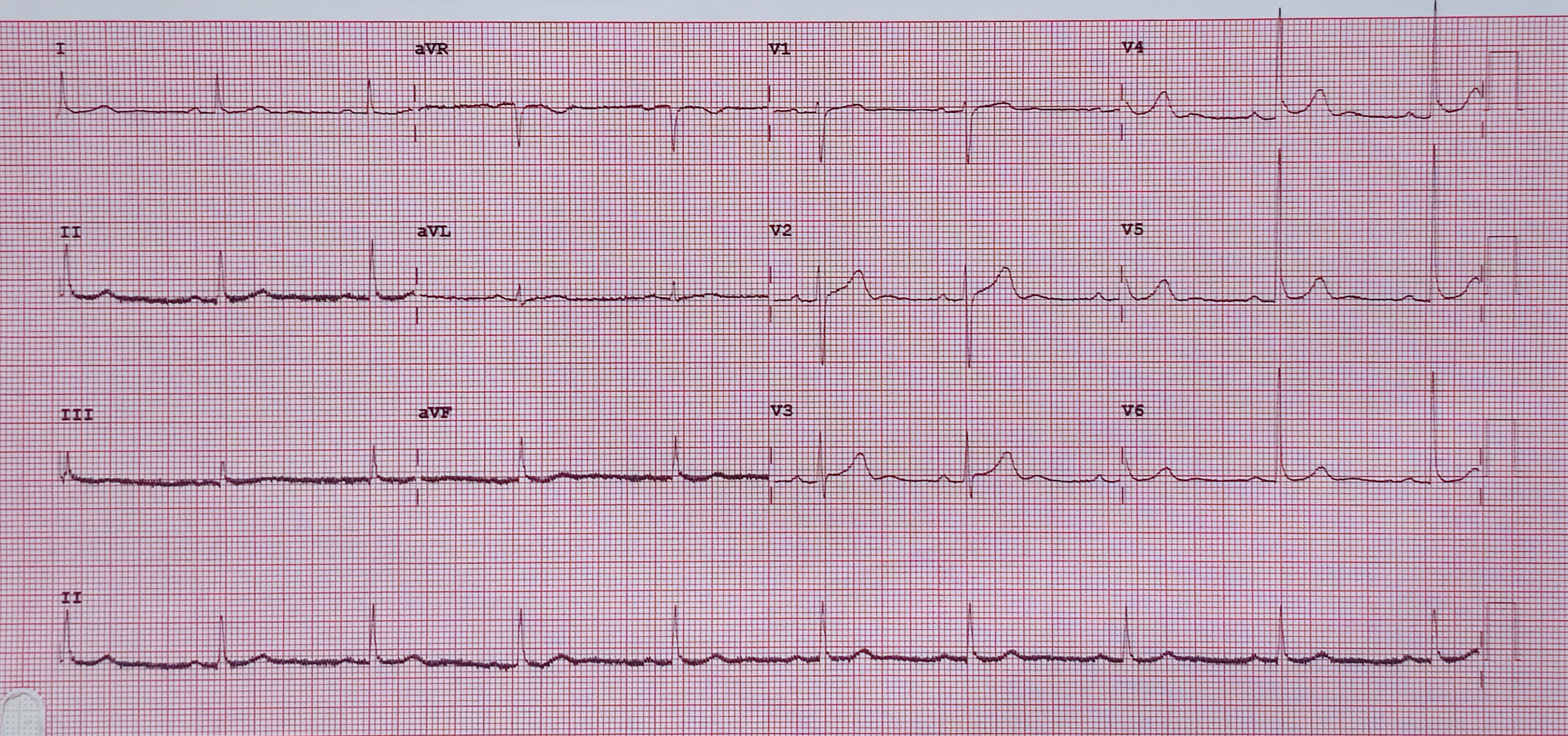
A 40-year-old gentleman, non-smoker with underlying Diabetes mellitus and Dyslipidaemia, was admitted for recurrent Unstable angina in late 2023. General examination showed HR 64 bpm, sinus rhythm, BP 118/64mmHg; lungs and CVS unremarkable. ECG on arrival showed sinus rhythm with no ST segment changes. He was admitted for Acute coronary syndrome treatment with DAPT and anti-coagulation.
Relevant Test Results Prior to Catheterization
Troponin I was not raised. Otherwise, other blood investigations are unremarkable. CXR showed clear lung fields with no cardiomegaly. Echocardiography showed LVEF 60-65% with no RWMA. Coronary angiography showed mild distal LM disease with mild proximal LAD disease, supplying Rentrop Grade 3 collaterals to PDA and proximal 30-50% disease of main diagonal. Proximal subtotal occlusion and distal CTO of non-dominant LCx and dominant RCA with diffuse proximal to mid 80-90% disease with distal CTO.
 LAD.mp4
LAD.mp4
LCx.mp4
RCA.mp4
Relevant Catheterization Findings
Right 6Fr trans-radial sheath used for contralateral access, LAD engaged with 6Fr EBU 3.5 guide catheter and a BMW guidewire passed into distal LAD. Right 7Fr trans-femoral sheath inserted and RCA engaged with 7Fr AL 0.75 guide catheter and bilateral contrast injection performed. Sion Blue gw with CorsairPro microcatheter support, passed into proximal-RCA and escalated to FielderXT-A, unable to cross proximal CTO, hence switched back to SionBlue and left in-situ. Switched to retrograde approach.
LAO.avi
RAO.avi
Antegrade Approach.avi
Interventional Management
Procedural Step
SionBlue with Caravel microcatheter advanced into midRCA,septal-surfing with Suoh03 through septo-epicardial collaterals. Caravel track through septal into PDA,escalated FielderXT-A,FielderXT-R,Pilot150, unable to puncture distal CTO cap.XT-R advanced into PDA and subintimal into proximalRCA via Knuckle wire technique. Antegrade GuidePlusII guide-extender (GE) to deliver NC2.0x15mm into proximalRCA,predilated proximalRCA. Proximal-midRCA predilated with NC3.0x15mm to assist retrograde entry with ReverseCART. Retrograde XT-R entered true lumen into antegrade GE,unable to cross retrograde Caravel. Antegrade CorsairPro with SionBlue waiting within GE,retrograde XT-R positioned into antegrade microcatheter within antegrade GE via Tip-in technique. Antegrade Corsair advanced over retrograde XT-R till distal to CTO while backingout retrograde Caravel. Antegrade Corsair advanced till distalPDA,SionBlue advanced into distalPDA,retrograde XT-R redrawn.Antegrade Corsair removed. Distal-midRCA predilated with NC2.0x15. Attempted wiring PLV with XT-A using Sidecar technique,unsuccessful d/t retroflexedPLV. ProximalPDA predilated with SC2.0x20. DistalRCA-proximalPDA stented with DES2.5x38mm, postdilated NC3.0x15. IVUS performed. Mid-distalRCA stented with DES3.0x38mm, ostial-proximalRCA with DES3.5x38mm,post-dilated NC3.5x15mm. OstialRCA POT NC4.5x8. PCI LCx,Suoh03 with Corsair advanced into distalLCx,predilated distal-proximalLCx with NC2.0x15 & Scoring2.5x15mm,treated with DCB2.5x40
Tip in technique.mp4
RCA final shot.mp4
LCx final shot.mp4
Case Summary
Tip-in or Rendezvous techniques can be used upfront rather than when Retrograde wire externalization (RWE) technique is unfeasible/undesirable after successful retrograde guidewire crossing. Sidecar technique with guidewire co-transporter represents a simple and inexpensive alternative solution to deliver a second guidewire distally once CTO is crossed, in suitable lesions. Use of DCBs in small vessel size, avoiding use of stents.