CASE20240815_002
A Challenging Case Report of Complex Critical Medina 1-1-1 Left Dominant Lcx PCI with Atypical Aslanger Pattern Guided Revascularization
By Petchlada Jansiriyotin
Presenter
Petchlada Jansiriyotin
Authors
Petchlada Jansiriyotin1
Affiliation
Rajavithi Hospital, Thailand1,
View Study Report
CASE20240815_002
Complex PCI - Bifurcation
A Challenging Case Report of Complex Critical Medina 1-1-1 Left Dominant Lcx PCI with Atypical Aslanger Pattern Guided Revascularization
Petchlada Jansiriyotin1
Rajavithi Hospital, Thailand1,
Clinical Information
Relevant Clinical History and Physical Exam
A Thai female 51 yrs patient; with T2DM, HTN, DLP and ESRD on regular hemodialysis without smoking; presented with chest discomfort for 14 hours prior to admission. Her BP was 165/112 mmHg, pulse rate was 110 bpm and pulse oxygen was 99% at room air. Her pain score was 4 out of 10.
Relevant Test Results Prior to Catheterization
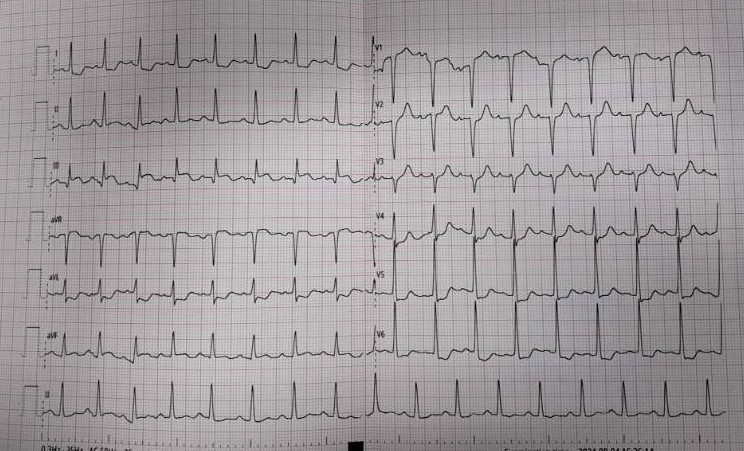
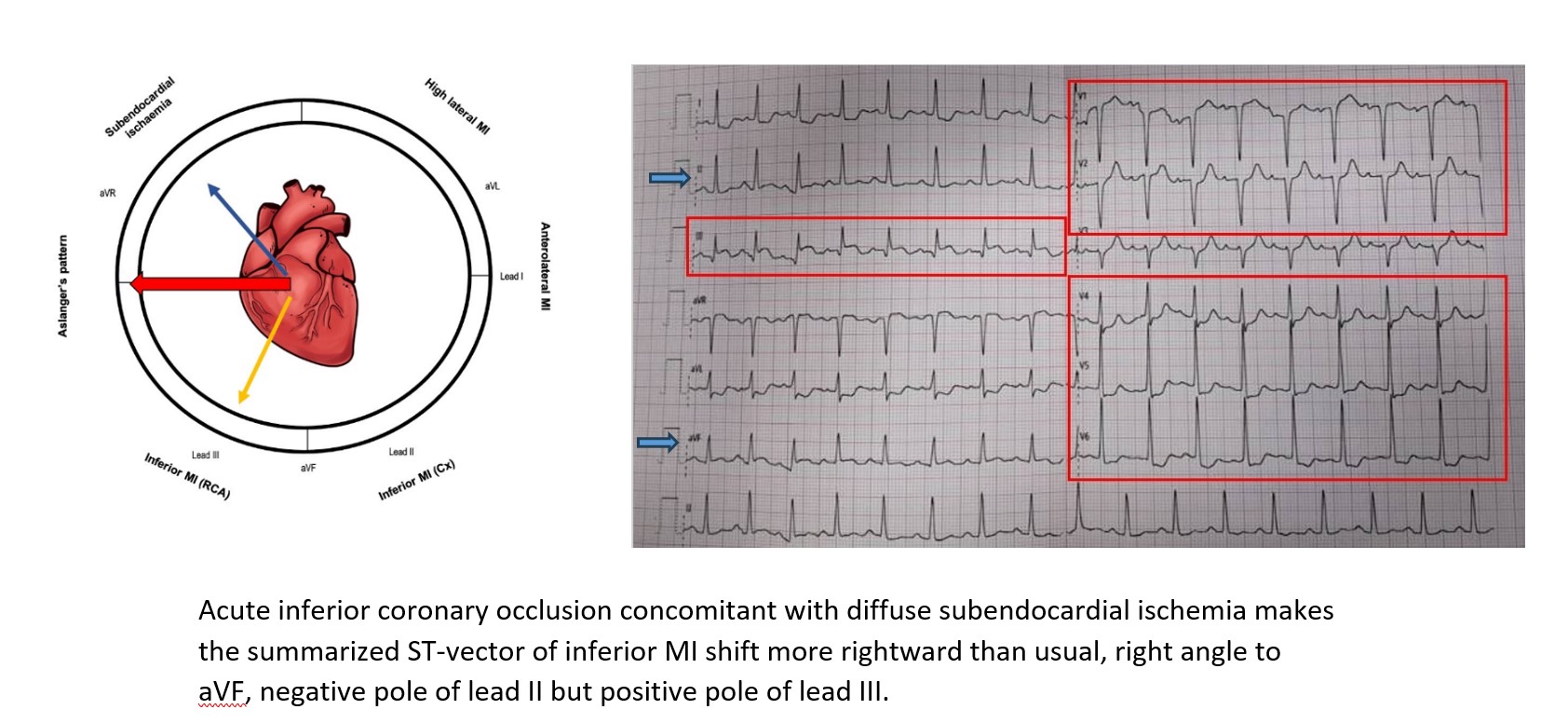
EKG showed STE III & aVR, Q wave V1-2, STD V4-6 & I & aVL compatible with Aslanger pattern. Echocardiogram bedside showed poor LV contraction, LVEF 45%, Hypokinesia at inferior wall, preserve RV function and no significant valvular heart disease.
Relevant Catheterization Findings
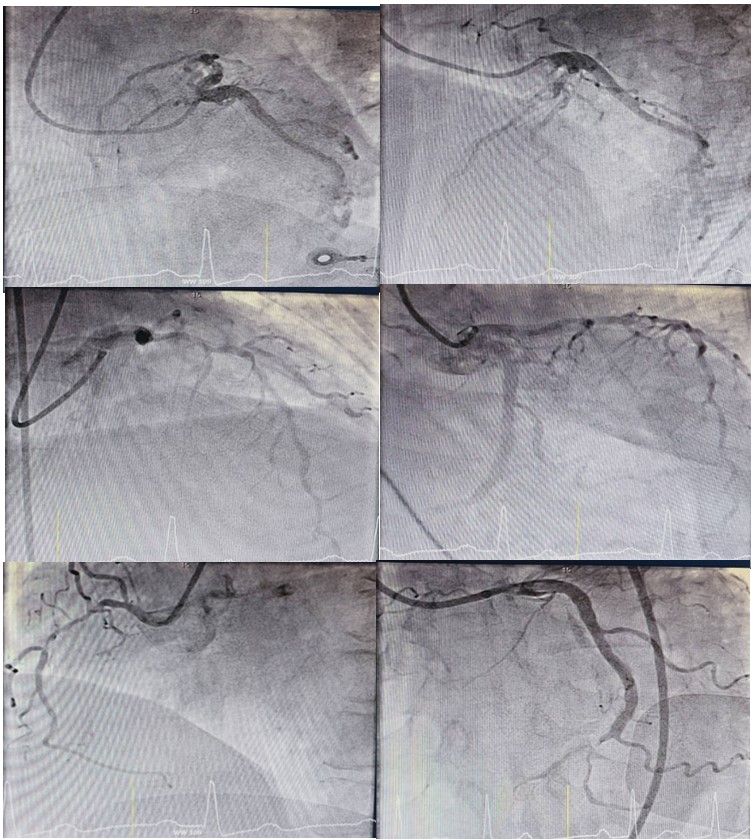
CAG via right femoral approach with diagnostic catheter 6Fr JL3.5 showed Left dominant vessel, LM : short LM without stenosis, LAD : 70% stenosis pLAD, 85% stenosis mLAD, LCx : 95% stenosis last OM with TIMI flow I-II, RCA : 70% stenosis mRCA. PCI of distal LCx with provisional stenting technique. GD : EBU 7 Fr 3.5. Turntrac with Finecross pass through distal LCx and OM. Predilate with SC balloon 2.0x15 mm. Firehawk 2.5x18 mm Deployed distal LCx 14 atm.
Interventional Management
Procedural Step
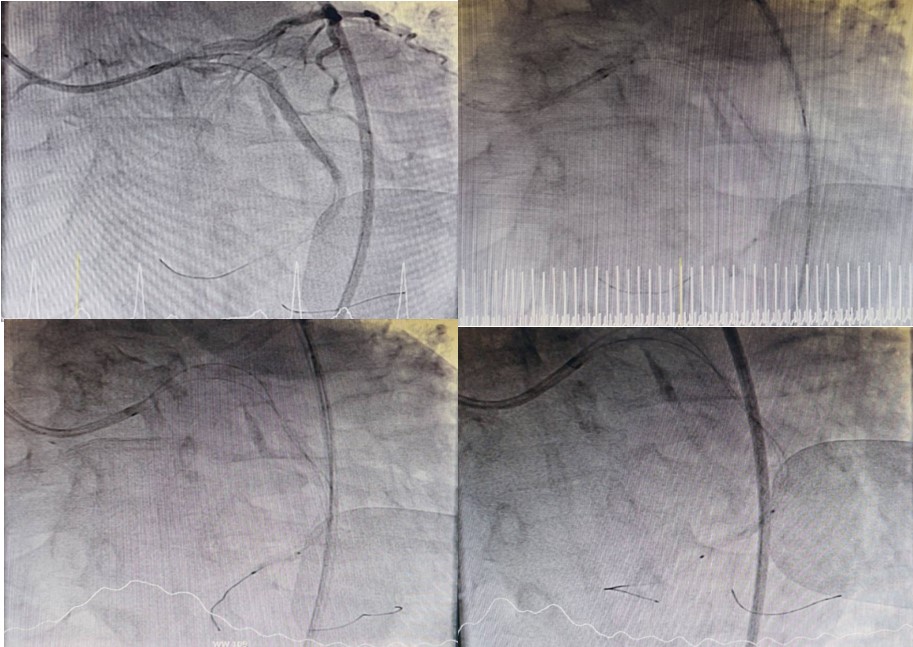
CAG via right femoral approach with diagnostic catheter 6Fr JL3.5 showed Left dominant vessel, LM : short LM without stenosis, LAD : 70% stenosis pLAD, 85% stenosis mLAD, LCx : 95% stenosis last OM with TIMI flow I-II, RCA : 70% stenosis mRCA. TVD with inferior wall STEMI was diagnosis. PCI of distal LCx with provisional stenting technique. Guiding : EBU 7 Fr 3.5. Guide wire : Turntrac with Finecross pass through distal LCx and OM. Predilate with SC balloon 2.0x15 mm. Firehawk 2.5x18mm Deployed distal LCx 14 atm. Final angiogram was acceptable result.
Case Summary
1.Although Aslanger pattern is not fulfilled STEMI criteria but a specific ECG pattern is concerning for acute inferior occlusion MI with concomitant multi-vessel disease and should be emergently evaluated for revascularization. 2.Concomittant critical stenosis on other coronary arteries in Aslanger pattern explains why infarct size and mortality have been rising.3.The Aslanger pattern in left dominant coronary was not common and should not delay treatment.4.Performing a simple PCI with a provisional stenting technique for Medina 1-1-1 bifurcation may be a suitable option to avoid adverse complications during high thrombogenicity STEMI PCI.