CASE20240814_001
Navigating the Triple Threat: Managing Triple Culprit STEMI
By Muhammad Isra Tuasikal, Dafsah Arifa Juzar, Siska Suridanda Danny, Doni Firman, Arwin Saleh Mangkuanom, Nanda Iryuza, Victor Giovannie Xaverison Rooroh, Dena Karina Firmansyah, Aris Munandar ZI, Amir Aziz Alkatiri
Presenter
Muhammad Isra Tuasikal
Authors
Muhammad Isra Tuasikal1, Dafsah Arifa Juzar1, Siska Suridanda Danny1, Doni Firman1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Victor Giovannie Xaverison Rooroh1, Dena Karina Firmansyah1, Aris Munandar ZI1, Amir Aziz Alkatiri1
Affiliation
National Cardiovascular Centre Harapan Kita, Indonesia1,
View Study Report
CASE20240814_001
ACS/AMI - ACS/AMI
Navigating the Triple Threat: Managing Triple Culprit STEMI
Muhammad Isra Tuasikal1, Dafsah Arifa Juzar1, Siska Suridanda Danny1, Doni Firman1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Victor Giovannie Xaverison Rooroh1, Dena Karina Firmansyah1, Aris Munandar ZI1, Amir Aziz Alkatiri1
National Cardiovascular Centre Harapan Kita, Indonesia1,
Clinical Information
Relevant Clinical History and Physical Exam
A 57 years old man came with chief complaint of severe chest pain since 18 hours before admission. Vital signs examination showed blood pressure was 65/42 mmHg and heart rate 81 bpm accompanied by cold extremities and signs of shock. Laboratory findings also showed increased HS-Troponin-T accompanied by metabolic acidosis. Double support inotropes, central venous line, and Intra-Aortic Balloon Pump was inserted.
 1.2.840.113619.2.478.196654532329441882.1722217354.14156.1084.dcm.wmv
1.2.840.113619.2.478.196654532329441882.1722217354.14156.1084.dcm.wmv
Relevant Test Results Prior to Catheterization
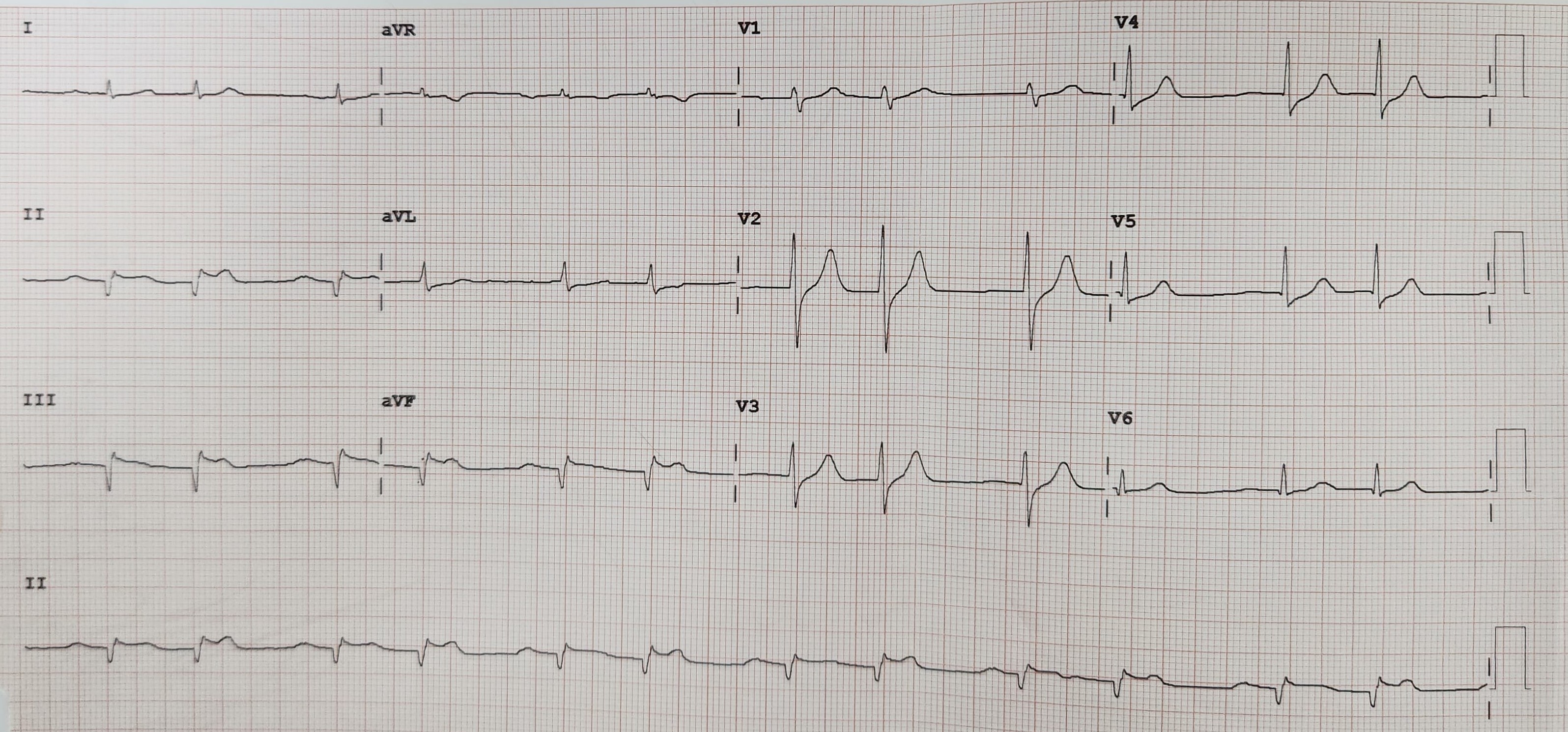
Electrocardiography showed ST Elevation at II III aVF and slight ST depression at V2-V4 with couplet premature atrial contraction. Echocardiography showed ejection fraction 30% (simpson’s), TAPSE 8 mm, positive regional wall motion abnormalities, and low cardiac output with high systemic vascular resistance which showed signs of cardiogenic shock due to acute coronary syndrome.
1.2.840.113619.2.478.196654532329441882.1722217354.14156.956.dcm.wmv
1.2.840.113619.2.478.196654532329441882.1722217354.14156.968.dcm.wmv
1.2.840.113619.2.478.196654532329441882.1722217354.14156.976.dcm.wmv
Relevant Catheterization Findings
Angiography showed thrombus grade V at proximal RCA, thrombus grade V at proximal LCx, total occlusion at mid LAD. Since the initial ECG showed inferior wall infarction, we decided to revascularize RCA. Workhorse wire successfully penetrated lesion and placed at distal RCA. Predilation was carried with SC balloon 2.5 x 15 mm from proximal – distal, but unfortunately TIMI flow remained 0 because of high thombus burden. Eptifibatide was then administered and the team decided to defer stenting
1.2.840.113619.2.478.196654532329441882.1722217354.14156.1018.dcm.wmv
1.2.840.113619.2.478.196654532329441882.1722217354.14156.1036.dcm.wmv
1.2.840.113619.2.478.196654532329441882.1722217354.14156.1060.dcm.wmv
Interventional Management
Procedural Step
After 3 days, we proceeded to re-attempt PCI. Angiography findings showed improvement flow TIMI I at RCA, TIMI I at LCx, and CTO LAD with collaterals from RCA. POBA RCA was done using floppy wire and SC Balloon 2.5 x20 mm from proximal – mid RCA, resulted in TIMI II flow with high thrombus burden. Proceeded to PCI CTO LAD using Fielder XT-A backup microcatheter but failed to penetrate the lesion at proximal. Escalating wire with Gaia Second successfully penetrated CTO lesion and placed to distal LAD. Exchange with floppy to distal LAD, continued with pre-dilatation with SC Balloon 2.5 x 15 mm from mid –proximal LAD, angiographic evaluation showed TIMI II flow with residual stenosis. Proceed to POBA LCx, POBA LCx was done using floppy wire and SC Balloon 2.5 x 20 mm from proximal –distal LCx, resulted in TIMI II Flow with high thrombus burden. We then proceeded to PCI LAD, using NC Scoreflex 3.0 x15 mm to predilate from distal –osteal LAD, followed by implantation of DES Xience 3.0 x 33 mm from osteal – mid LAD. Post-dilatation was performed using NC Balloon 3.5 x 10 mm at proximal stent, and the evaluation showed TIMI III flow but with residual stenosis at distal LAD. POBA with SC Balloon 2.5 x 15 mm was performed at distal LAD, and the angiography evaluation showed TIMI III Flow. Final result was TIMI III Flow LAD, TIMI II Flow LCx, and TIMI II Flow RCA, with high thrombus burden at RCA and LAD.
Screen Recording 2024-08-14 134310.mp4
Case Summary
PCI in STEMI is always difficult to predict. It could be straightforward, but also occasionally it became very complex. Managing triple culprit with critical conditions such as cardiogenic shock and high thrombus burden has its own difficulties. Circulatory support either by mechanical and drugs are necessary to improve and stabilize the patient. Due to the complexity of the lesions, patient's condition, and every possible effort has been done during initial emergency PCI, we decided to defer the stenting procedure, as soon there was improvement. Re-attempt PCI was then carried out 3 days later with much better preparations and the optimal result was then achieved.