CASE20240813_003
A Case of Type 4 Perforation with IVL in a Very Small Calibre Calcified LAD
By Rohit Mody
Presenter
Rohit Mody
Authors
Rohit Mody1
Affiliation
Mody Harvard Heart Institute & Research Centre. Bathinda, Punjab, India1,
View Study Report
CASE20240813_003
Complication Management - Complication Management
A Case of Type 4 Perforation with IVL in a Very Small Calibre Calcified LAD
Rohit Mody1
Mody Harvard Heart Institute & Research Centre. Bathinda, Punjab, India1,
Clinical Information
Relevant Clinical History and Physical Exam
A-72-years male, acute anterior wall MI 1-month back went toa nearest hospital with Cathlab capabilities. A diffuse LAD disease sent backafter just a POBA by history and angiogram. When I received patient LM andcalcified and diffuse LAD slow distal flow and calcified also Clinicallypatient throwing VT and AF episodes.

Relevant Test Results Prior to Catheterization
A-72-years male, acute anterior wall MI 1-month back went toa nearest hospital with Cathlab capabilities. A diffuse LAD disease sent backafter just a POBA by history and angiogram. When I received patient LM andcalcified and diffuse LAD slow distal flow and calcified also Clinicallypatient throwing VT and AF episodes.
Relevant Catheterization Findings
During angiogram the earlier borderline haemodynamics ofpatient became still intense inotropes started and IABP inserted EF 18%Creeping into cardiogenic shock
Interventional Management
Procedural Step
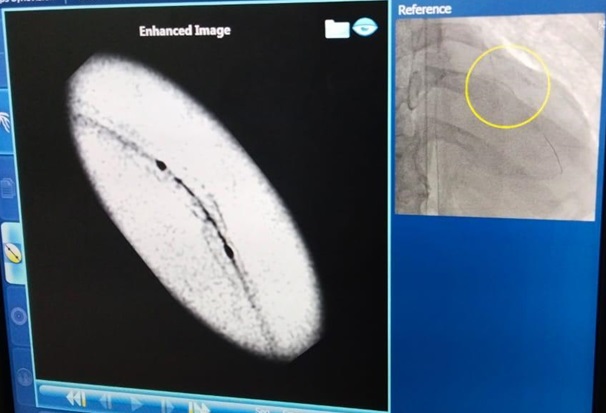
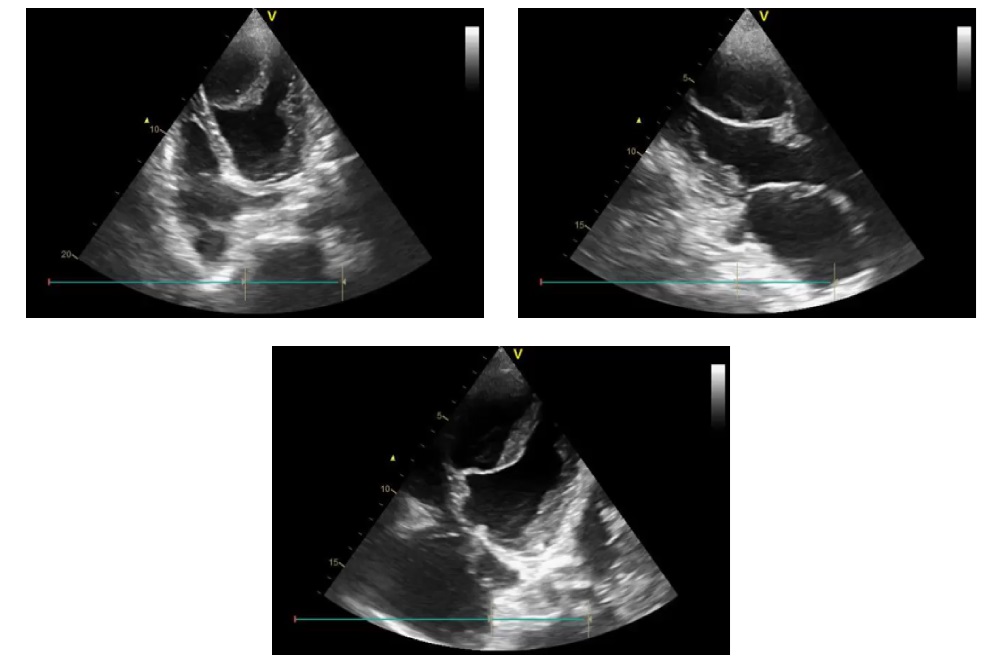
There is dissection in proximalLAD and there is significant LM ostial and distal disease. Angiogram might notbe showing how calcified LAD even distal diffuse disease is actually calcifiednot a ECG favouring CRTD insertion. No option but to go in forrevascularisation. For the response planned with Impella. Relatives reluctantdue to the cost. angioplasty on IABP support really understanding about riskprognosis. patient on cardarone now a bit settled arrhythmias. Because ofdissection tried with Fielder FC went to diagonal requiring fiddling at bend sochanged to BMW could negotiate till apex. Took 2 mm balloon difficulty goes into distalsegment Distal segment doesn’t expand much even 2.5 mm balloon and IVUS notgoing decided to stent proximal LAD, Another stent 3.5 mm at 24 ATM in LM, Therewas still a dissection in the distal part, A calcified spur at distal stent 3stent. To be perfect IVL to distal stent, After IVL 2.5 mm this was resultlarge perforation, It is coronary to LV fistula with flow will occur only indiastole. Patient stable on IABP Should we continue IABP or it iscontraindicated. Coiling might cause distal embolism in LV or proximal stentthrombosis when distal run of 2 proximal stents is closed. Patient still doingwell 5 days old echocardiogram. We decided conservatively patient can do wellinstead of coiling device closure or if we are lucky to get covered stentacross. Patient was in bad state be

Case Summary
Retrospectively I feel if I hadstopped where I used IVL there would have been definitely gain to patient. Buteverything is not in your hands we don’t get complications with our will theyhappen. In 100 odd usage of IVL this was our first case perforation with IVL. Aballoon to vessel ratio of 1:1 is ideal scenario for IVL Here I could notinsert eagle eye and used smallest possible balloon went up to 6 ATM Stilloccurred and it was at stent edge probably already weakened by high pressure mvinflation to crack the calcified spur rock on bottom. Calcified distal vesselswhich are small calibre also always pose a bigger threat.