CASE20240812_001
Drug-Coated Balloon Combined with Provisional Drug-Eluting Stent Implantation for the Treatment of De Novo Medina 010 Main Coronary Bifurcation Lesions
By Yaojun Zhang, Wenrui Ma, Qingyuan Chen, Sili Feng
Presenter
Yaojun Zhang
Authors
Yaojun Zhang1, Wenrui Ma1, Qingyuan Chen1, Sili Feng1
Affiliation
Xuzhou New Health Geriatric Hospital, China1,
View Study Report
CASE20240812_001
Complex PCI - Bifurcation
Drug-Coated Balloon Combined with Provisional Drug-Eluting Stent Implantation for the Treatment of De Novo Medina 010 Main Coronary Bifurcation Lesions
Yaojun Zhang1, Wenrui Ma1, Qingyuan Chen1, Sili Feng1
Xuzhou New Health Geriatric Hospital, China1,
Clinical Information
Relevant Clinical History and Physical Exam
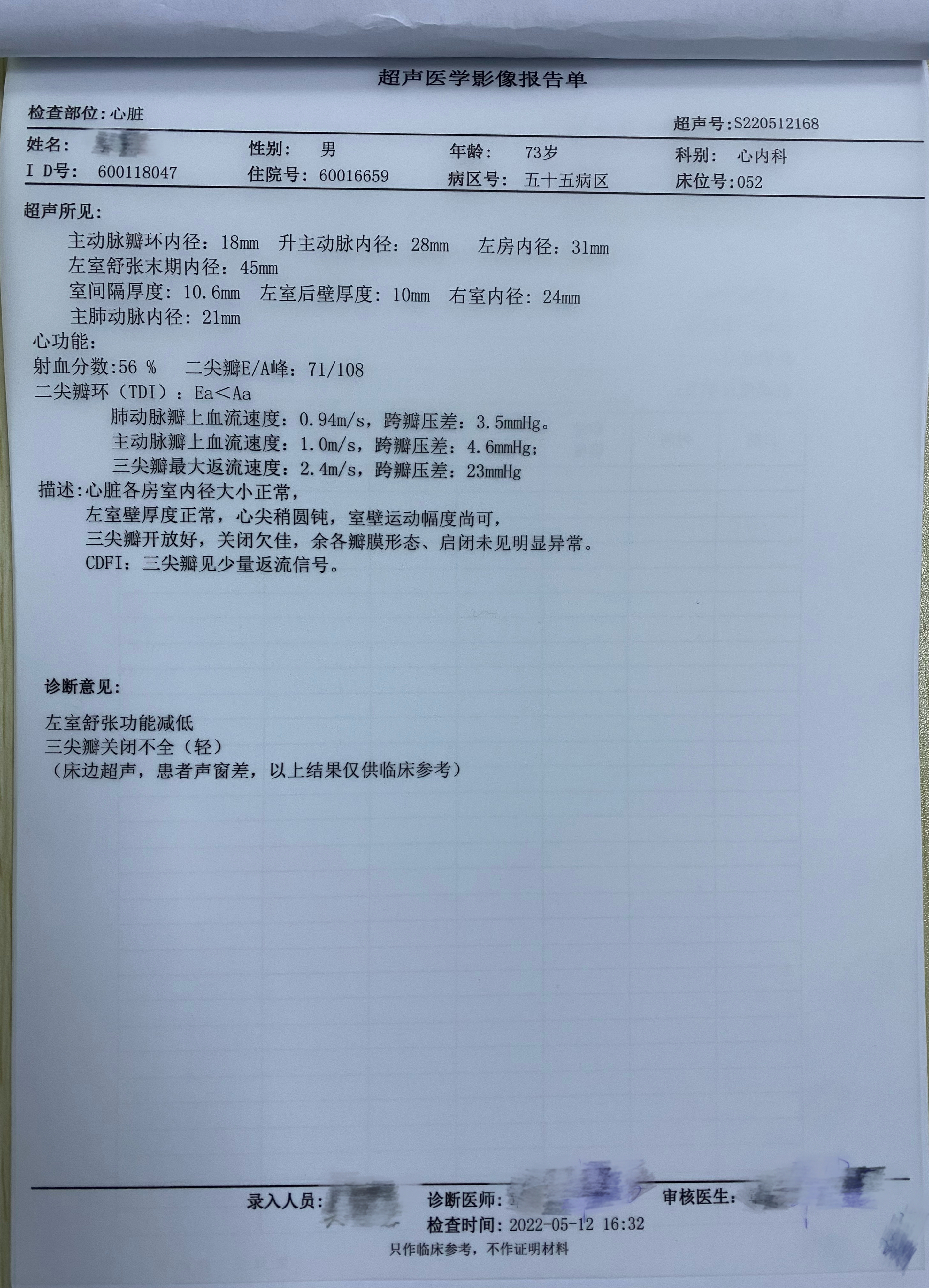
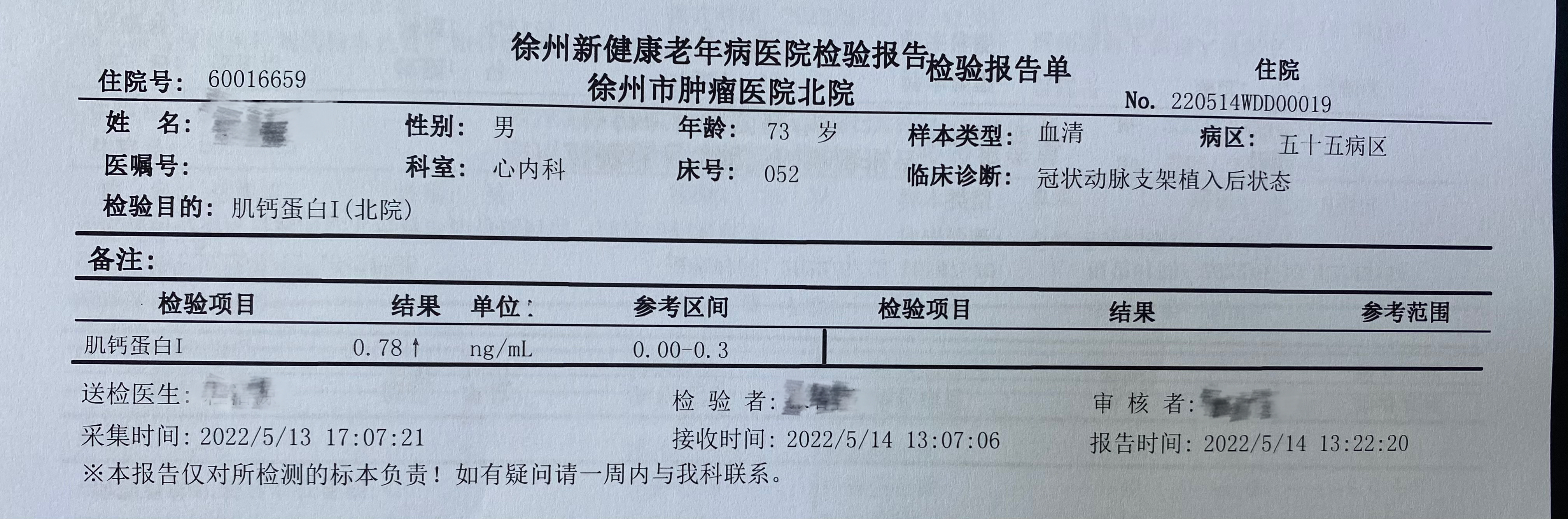
A 73-year-old male was admitted to our hospital because he had experienced chest pain in the past 2 days. The electrocardiography(ECG) showed QS wave in ECG leads V1 - V3, and Troponin I elevated to 0.78 ng/mL. The patient had been smoking and had a history of diabetes mellitus for more than 20 years. The results of echocardiography indicated that the patient had mild tricuspid valve insufficiency and left ventricular hypo-diastolic function with an ejection fraction of 56%.
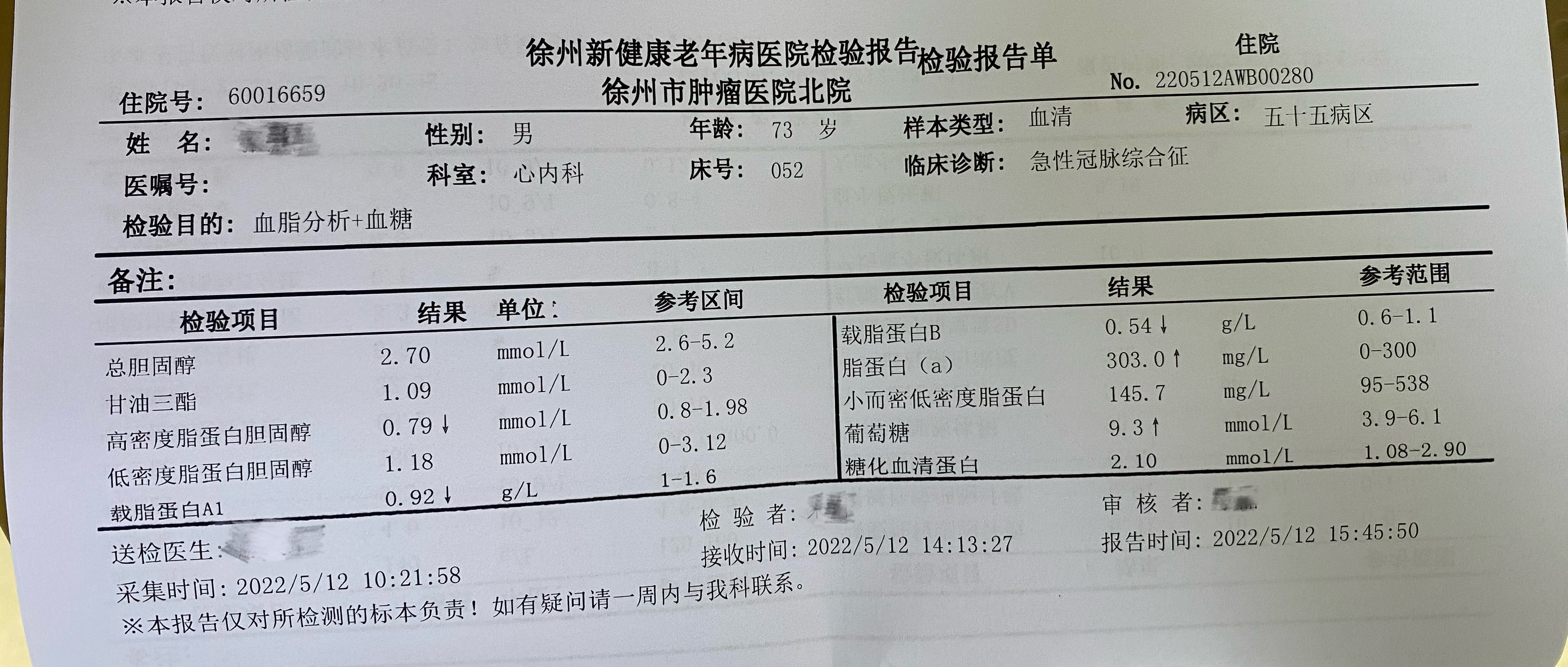
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
Angiography revealed a Medina 010 bifurcation lesion – the left main is normal; the ostium and proximal stenosis of the left anterior descending artery (LAD) is 90%, mid-segment stenosis 70%, and distal stenosis 80%; the circumflex artery (LCX) is diffusely stenotic, with the most severe stenosis being 85%. A 6-French SPB 3.5 guiding catheter (Asahi Intecc Co., Ltd., Japan) was inserted from the right radial artery. First, we performed the pre-dilatation of LCX with a 2.0 mm × 20 mm balloon and implanted 2.5 mm × 29 mm (Firehawk, MicroPort Inc., China) at the mid segments. Then, we failed to deliver the 2.25 × 24 mm (ExCrossal, JW Medical Systems, China)stent to the distal segment and thus switched to implanting a 2.25 × 13 mm (Firehawk, MicroPort Inc., China) stent. Next, a Sion guide wire (Asahi InteccCo., Ltd., Japan) was successfully introduced into the distal of LAD. This mid-segment of LAD was pre-dilated with the 2.5 mm × 20 mm (Pioneer, MicroPort Inc., China)plain balloon, and implanted 2.75 mm × 19 mm (ExCrossal, JW Medical Systems, China). After that, a cutting balloon (2.75 mm × 15 mm) (Flextome, Boston Scientific Co., USA) was employed to dilate the ostium of LAD. Subsequently, a 2.75mm × 30 mm drug-coated balloon (DCB) (SeQuent Please, B Braun Melsungen AG, Germany) was performed at 6 atm for 35 s to treat this lesion. Finally, a drug-eluting stent (2.75 mm × 24 mm) (ExCrossal, JW Medical Systems, China) was implanted 1-2 mm distally to the ostium of LAD.
 Procedural step.wmv
Procedural step.wmv
Case Summary
The present findings suggest that DCB combined with provisional DES implantation, which is located in the 1-2 mm distally to the de novo medina 010 main coronary bifurcation lesions, could be an alternative revascularization therapy of choice.