CASE20240811_002
Left Main Bifurcation Disease with a CTO of LAD a Spectrum of Challenges Overcome
By Thomas George
Presenter
Thomas George
Authors
Thomas George1
Affiliation
Caritas Heart Institute, India1,
View Study Report
CASE20240811_002
Complex PCI - Bifurcation
Left Main Bifurcation Disease with a CTO of LAD a Spectrum of Challenges Overcome
Thomas George1
Caritas Heart Institute, India1,
Clinical Information
Relevant Clinical History and Physical Exam
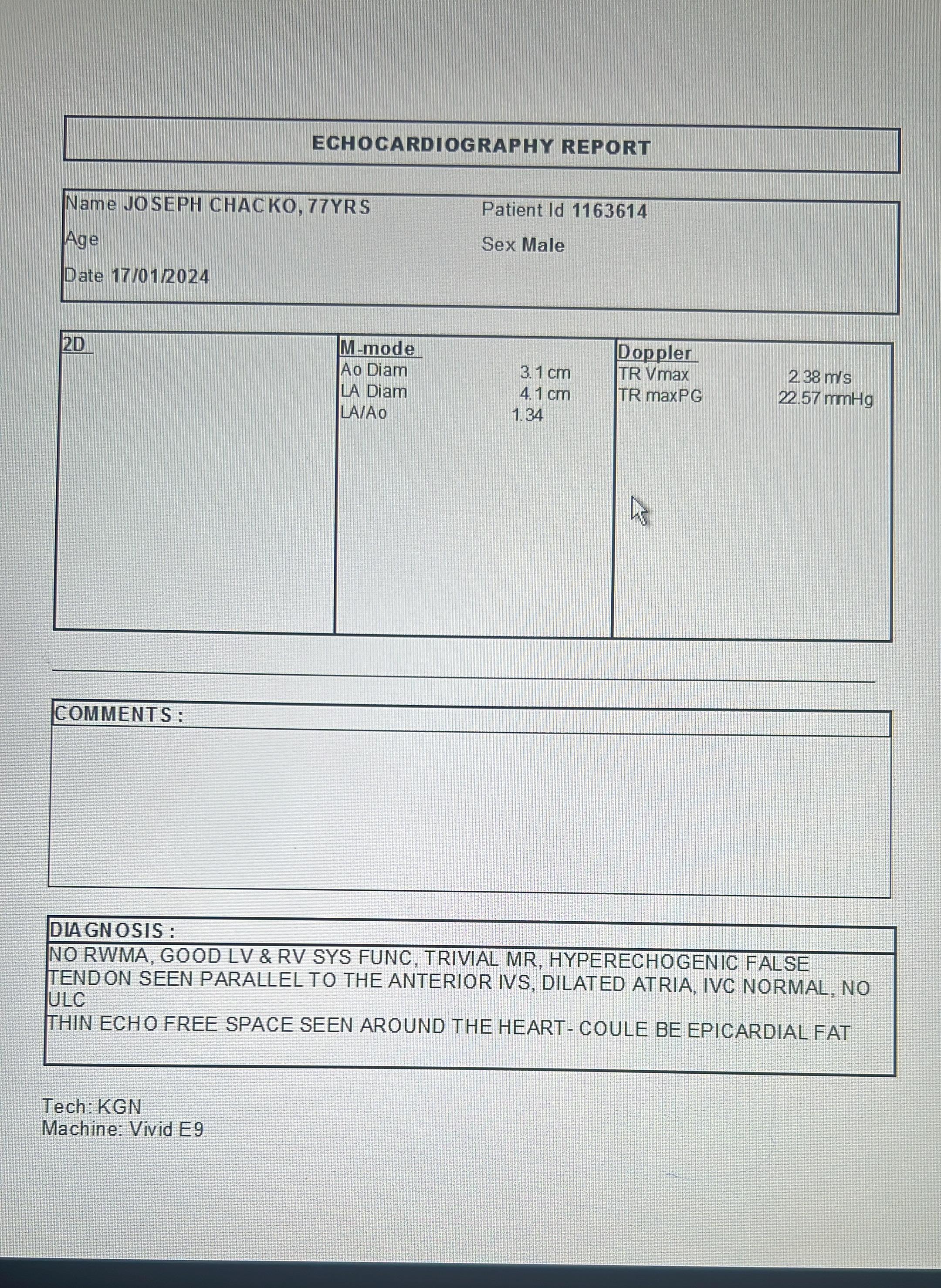
77 year old gentleman presented with class 2 effort dyspnoea & pre-syncope to local hospital. He had no prior history of diabetes/Hypertension or stroke in past. His physical examination did not reveal any major abnormalities
Relevant Test Results Prior to Catheterization
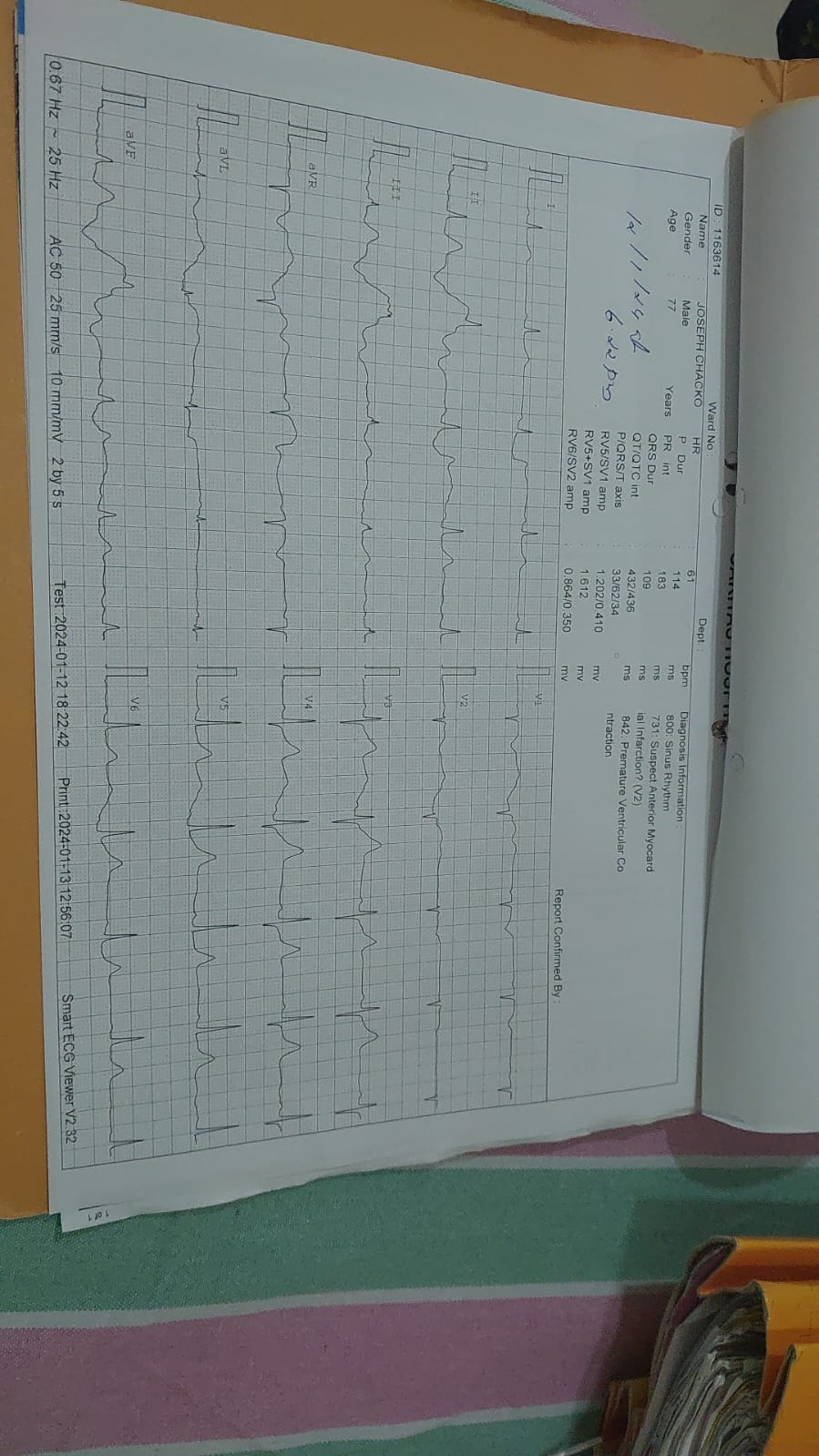
Ecg-sinus bradycardia & Echo-dilated Left Atrium with no significant valvular abnormalities or regional wall motion abnormalities
Relevant Catheterization Findings
critical left main bifurcation disease .CTO of LAD Rca was normal
 mov-series-032-Coronary.wmv
mov-series-032-Coronary.wmv
mov-series-002-Coronary_00001.wmv
mov-series-005-Coronary_00001.wmv
Interventional Management
Procedural Step
our access was Rt Femoral with a 7 Fr EBU Guide. The CTO in proximal LAD was crossed with a GAIA 2 wire with microcatheter support. The wire in true lumen was confirmed through retrograde injection through Rt coronary artery.The lesion was serially predilated with 1.5x 10.2.5 x 15 nc balloons. We then did an IVUS study of LAD after replacing the GAI 2 wire with runthrough wire . From distal to proximal LAD 3 DES,2.5x38,3.0x18 & 3.5x 48 were deployed with overlap & post dilated appropriately The proximal LAD stent was deployed with 2-3 struts protruding into Lt Main at the same time keeping a 4.0x15 nc balloon from Lt Main to LCX. The LAD stent was crushed with the 4.0 x15 nc balloon from LM to LCX. The LAD stent was then recrossed proximally & struts opened up with 2.5x 15 nc balloon..The proximal LAD stent was again post dilated .Next sequential dilatation at high pressures followed by first skb was done with 3.5 x15 Nc balloons in LAD & LCX .A 4.0 x 28 DES was deployed from Lt main to LCX. & pot done in Lt MAIN. The 2 nd recross was done proximally with 0.014 runthrough wire & struts opened with 2.5 x 15 nc balloon.Sequential dilatation of LAD & LCX followed by 2nd skb was done with 4.0 x 12 NCB inLM to LAD & 4.5 x12 NCB in LM to LCX.Final POT was done in Lt Main with 5.0 x 12 NCB in Left Main
mov-series-063-Coronary.wmv
mov-series-041-Coronary_00002.wmv
mov-series-068-Coronary.wmv
Case Summary
The CTO of lad was successfully crossed with GAI 2 wire with microcatheter support & wire position confirmed through retrograde RCA injection. IVUS helped confirm position of wire in true lumen & also to determine sizing of stents ,adequet lesion preperation & landing zones.A 2 stent strategy with DK crush was used .Post procedure OCT confirmed well apposed & well expanded stents with good MSAs.