CASE20240809_007
A Challenging Case that Performed PCI for Triple Vessel Disease Patient with Chronic Total Occlusion
By Yasusuke Kinoshita, Atsunori Okamura, Kota Tanaka
Presenter
Yasusuke Kinoshita
Authors
Yasusuke Kinoshita1, Atsunori Okamura1, Kota Tanaka1
Affiliation
Sakurabashi Watanabe Advanced Healthcare Hospital, Japan1,
View Study Report
CASE20240809_007
Complex PCI - Multi-Vessel Disease
A Challenging Case that Performed PCI for Triple Vessel Disease Patient with Chronic Total Occlusion
Yasusuke Kinoshita1, Atsunori Okamura1, Kota Tanaka1
Sakurabashi Watanabe Advanced Healthcare Hospital, Japan1,
Clinical Information
Relevant Clinical History and Physical Exam
A patient is a male in 50 s. The patient had the chest pain symptom on effort from one year ago.He came to accept chest pain frequently from three months ago.He had abnormal electrocardiogram pointed out by a medical examination andconsulted a nearby clinic.A coronary heart disease was doubted, and he became the introduction to ourhospital.He consults our hospital to June 26 , 2024 for the first time.
 長軸像.mp4
長軸像.mp4
Relevant Test Results Prior to Catheterization
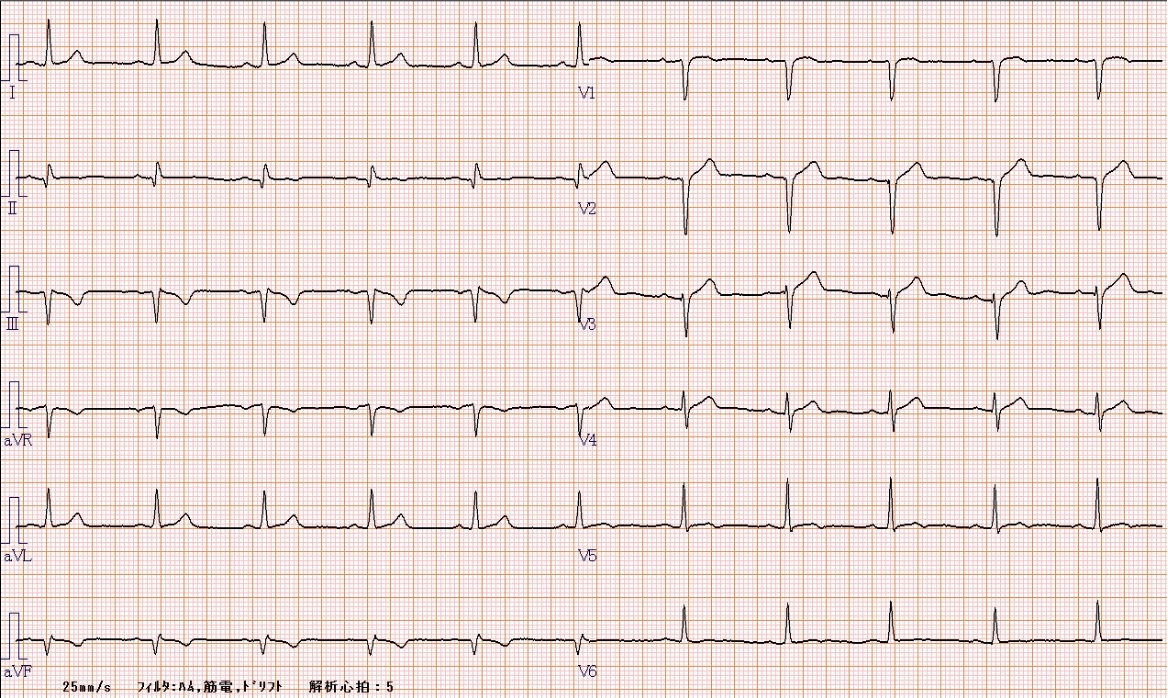
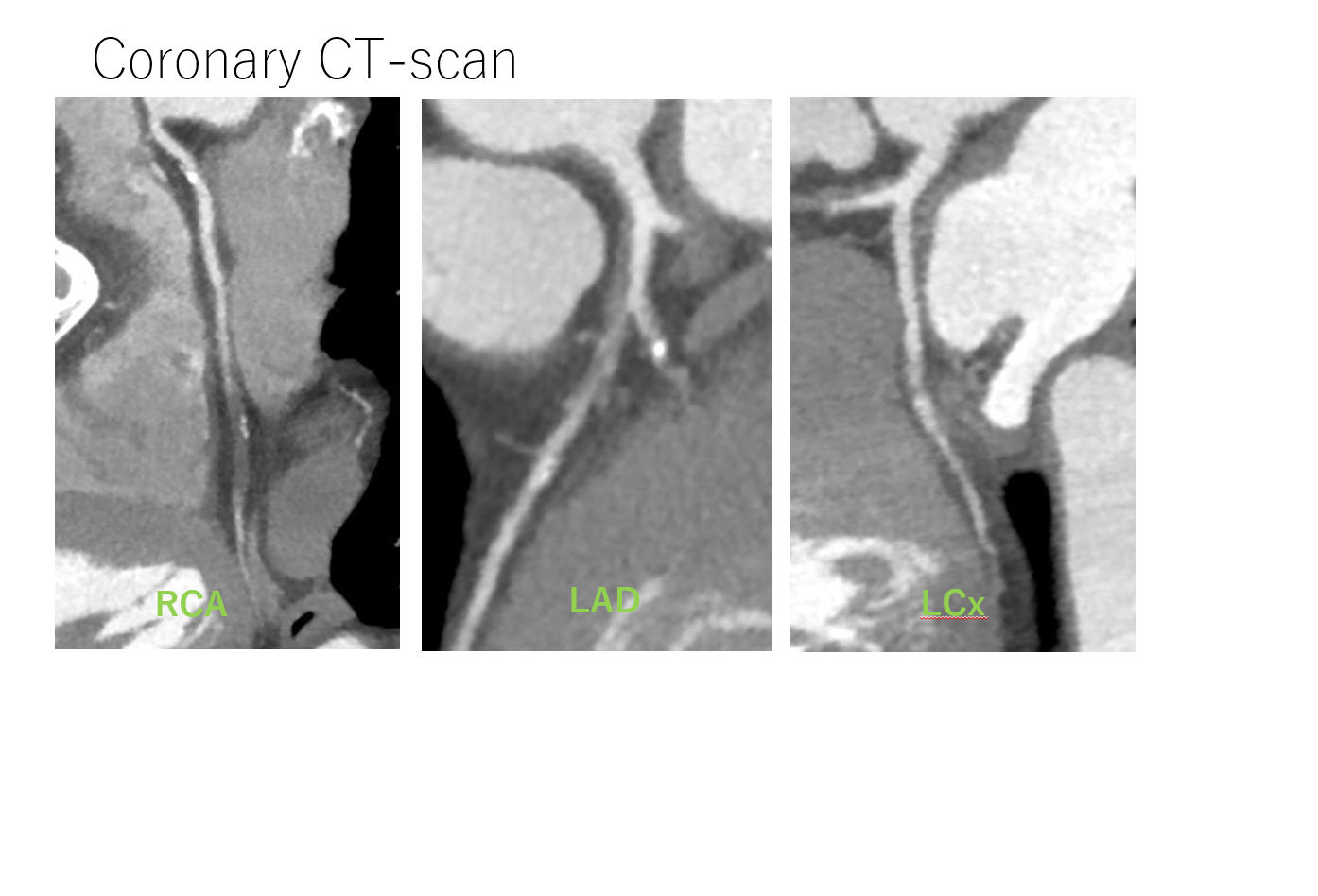
ECG shows abnormal q and negative T inⅡ,Ⅲ,aVf , and poor R in V 1 to V 3. Chest X-ray was not any problem.There is no abnormal finding by the blood test.There was views of mid-apical anterior hypokinesis by the cardiac echo check and Ejection Fraction was 50 %.It was CTO in middle RCA by the coronary CT-scan.Proximal LAD was a view to doubt obstruction and detected a severe stenosis lesion in middle LCx.
短軸像.mp4
CAG RCA LAO.MPG
Relevant Catheterization Findings
We performed first CAG to June 27, 2024.Middle RCA was CTO. We detected the collateral branch flow from RV branch in distal RCA.Middle LCx was tandem severe stenosis lesions.Proximal LAD was sub total occlusion. We detected the fair collateral branch flow from diagonal branch in distal LAD.There are triple vessel disease with RCA-CTO and LAD sub total lesion.
CAG RCA RAOCAU.MPG
CAG LAD CAU.MPG
CAG LAD CRA.MPG
Interventional Management
Procedural Step
We decided to treat LAD sub total lesion. Approach site was Right femoral artery, we insert 7 Fr sheath.Guiding catheter was EBU 3.5 SH. We observed LAD-lesion entrance in IVUS through SION wire to 1 st Diagonal branch which bifurcated from this side of the lesion.We used IVUS guide Tip detection method to pass a wire. We succeeded in wiring to LAD lesion using XT-R , Gaia Next 1 wire with Corsair pro.After observing it in IVUS, wire passed in LAD true lumen.Septal branch and 2 nd diagonal branch bifurcated a lesion from the inside, both were jailed by a plaque partition.In the same way, we use IVUS guide Tip-detection method to pass a wire for side branch.We passed a wire in Septal branch and 2 nd diagonal branch to protect a branch.We expanded it using semi-compliant balloon and scoring balloon from the LAD distal lesion.We expanded LAD and 2 nd diagonal branch bifurcation in KBT. We deployedstent Ultimaster Tansei 2.75 x 13 mm for LAD lesion.Because we recognized stent malapposition in IVUS, it performed post dilatation. Using micro catheter Sasuke, We passed SION wire again to 1 st diagonal branch which jailed stent.We expanded LAD and 1 st diagonal branch bifurcation in KBT. There is no stent malappositonin in final IVUS.
PCI CTO tip detection.MPG
IVUC CTO tip detection.MPG
PCI LAD final angio.MPG
Case Summary
We succeeded in passing a wire using theTip-detection method to true lumen for LAD sub total lesion.The side branch in the lesion did wire protection using the Tip-detection method and avoided occlusion.We performed PCI for triple vessel disease with the CTO and succeeded.