CASE20240809_006
Hybrid Approach in Treating Left Main Trifurcation Lesions
By Ivan Tsang
Presenter
Ivan Tsang
Authors
Ivan Tsang1
Affiliation
Princess Margaret Hospital, Hong Kong, China1,
View Study Report
CASE20240809_006
Complex PCI - Left Main
Hybrid Approach in Treating Left Main Trifurcation Lesions
Ivan Tsang1
Princess Margaret Hospital, Hong Kong, China1,
Clinical Information
Relevant Clinical History and Physical Exam
The patient was a 83 years old lady with history of bilateral breast cancer and colon cancer with operation done. She also had CRHD and AF with ECHO in 2023 showed an impaired LVEF 40% with mild MS and MR.She was admitted in May 2024 for acute decompensation of heart failure who presented with SOB and lower limb edema.P/E showed SpO2 91% on 2L O2 and respiratory distress. The BP was 166/118mmHg and fast AF with rate around 120bpm. Pitting edema was noted up to both knees.
 ECHO01.avi
ECHO01.avi
Relevant Test Results Prior to Catheterization
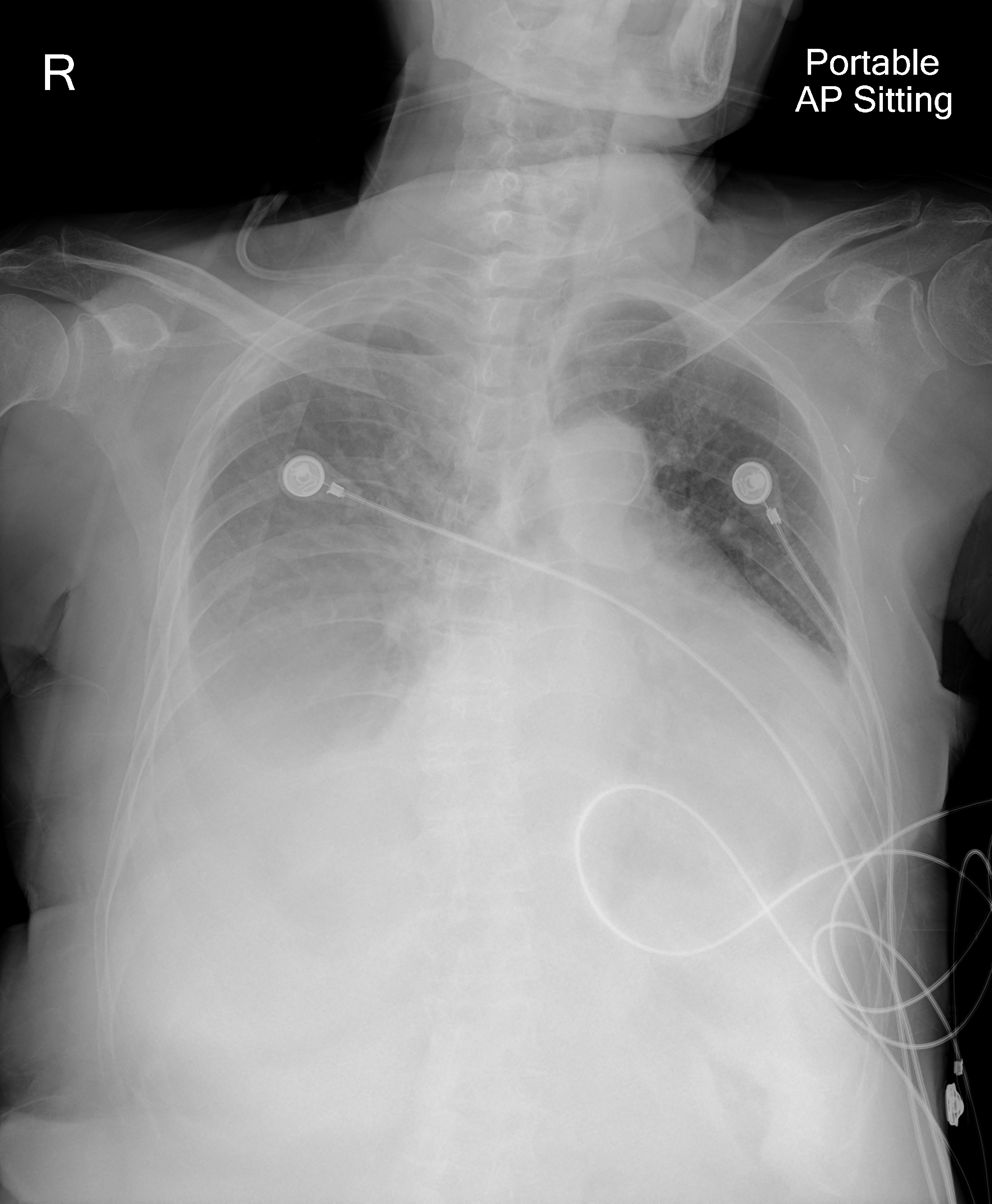
CXR showed bilateral pleural effusionECG showed fast AF and ST depression over precordial leadsBlood test showed elevated Troponin I level up to 2152ng/LBedside ECHO showed LVEF around 30-40% with mild MR / MS and rim of pericardial effusion
Relevant Catheterization Findings
Urgent CAG was performed with the following findings:dLM trifurcation lesion 90%oLAD 90%, mLAD 70%o/pRamus 90%oLCx subtotal occlusion (relatively small in size compared with Ramus)p/mRCA 30%
PA caudal.avi
RCA.avi
Interventional Management
Procedural Step
IABP was inserted via left femoral artery for mechanical circulatory supportPlan DCB to LCx and DK Culotte to LAD / Ramus bifurcation (Crush technique was not considered to avoid potential 3 layers of stent covering the ostium of LCx)R femoral approach; LM was engaged with 7F EBU 3.5 and wired to LAD / Ramus / LCx using Runthrough / Sion Blue / Sion respectivelyPTCA with SC 2.0 balloon and Wolverine 2.5x6IVUS to all 3 vessels was doneRamus and LAD were further pre-dilated with NC 3.0 balloonDCB (Sequent Please 2.5x20) to o/pLCxPTCS to LM-Ramus with Ultimaster Nagomi 2.5x24; Post dilated with NC 3.0 and POT with NC 4.0LAD and LCx were rewired and open strut with 2.5 balloonFirst kiss to LAD and Ramus using two NC 3.0 balloonsPTCS to LM-LAD with Ultimaster Nagomi 2.5x50; post dilated with NC 2.5, NC 3.0 and POT with NC 4.0 balloonLCx and Ramus were rewired and open struct with 2.5 balloonSecond kiss to LAD / Ramus with two 3.0 balloonsfinal IVUS and angio showed satisfactory results
Post PA caudal.avi
Post PA cranial.avi
wiring.avi
Case Summary
The patient showed satisfactory recovery after the procedure and CXR showed resolution of pulmonary congestion. She was put on DAPT and NOAC (for AF stroke prophylaxis) and so far no clinical bleeding side effect. She was given a course cardiac rehab and eventually discharged from hospital with total length of stay around 1.5 months.
This case demonstrated the possibility of hybrid approach in treating trifurcation lesion using DCB and DES in order to avoid complex '3 stents strategy'.
This case demonstrated the possibility of hybrid approach in treating trifurcation lesion using DCB and DES in order to avoid complex '3 stents strategy'.