CASE20240807_005
An Unusual Cause of Left Main Disease
By Thinnakrit Sasiprapha, Krissada Meemook, Thanaphruet Issarawattana
Presenter
Thinnakrit Sasiprapha
Authors
Thinnakrit Sasiprapha1, Krissada Meemook1, Thanaphruet Issarawattana2
Affiliation
Ramathibodi Hospital, Thailand1, Maharaj Nakhon Si Thammarat Hospital, Thailand2,
View Study Report
CASE20240807_005
Complex PCI - Left Main
An Unusual Cause of Left Main Disease
Thinnakrit Sasiprapha1, Krissada Meemook1, Thanaphruet Issarawattana2
Ramathibodi Hospital, Thailand1, Maharaj Nakhon Si Thammarat Hospital, Thailand2,
Clinical Information
Relevant Clinical History and Physical Exam
A 71-year-old male presented with progressive dyspnea and chest tightness on exertion for 2 months, FC II > FC III. He reported no orthopnea, paroxysmal nocturnal dyspnea (PND), edema, or chest pain. Physical examination revealed a regular heart rate, parasternal heaving, normal S1, and a loud P2. Additionally, a grade II pansystolic murmur was auscultated at the left lower parasternal border.

Relevant Test Results Prior to Catheterization
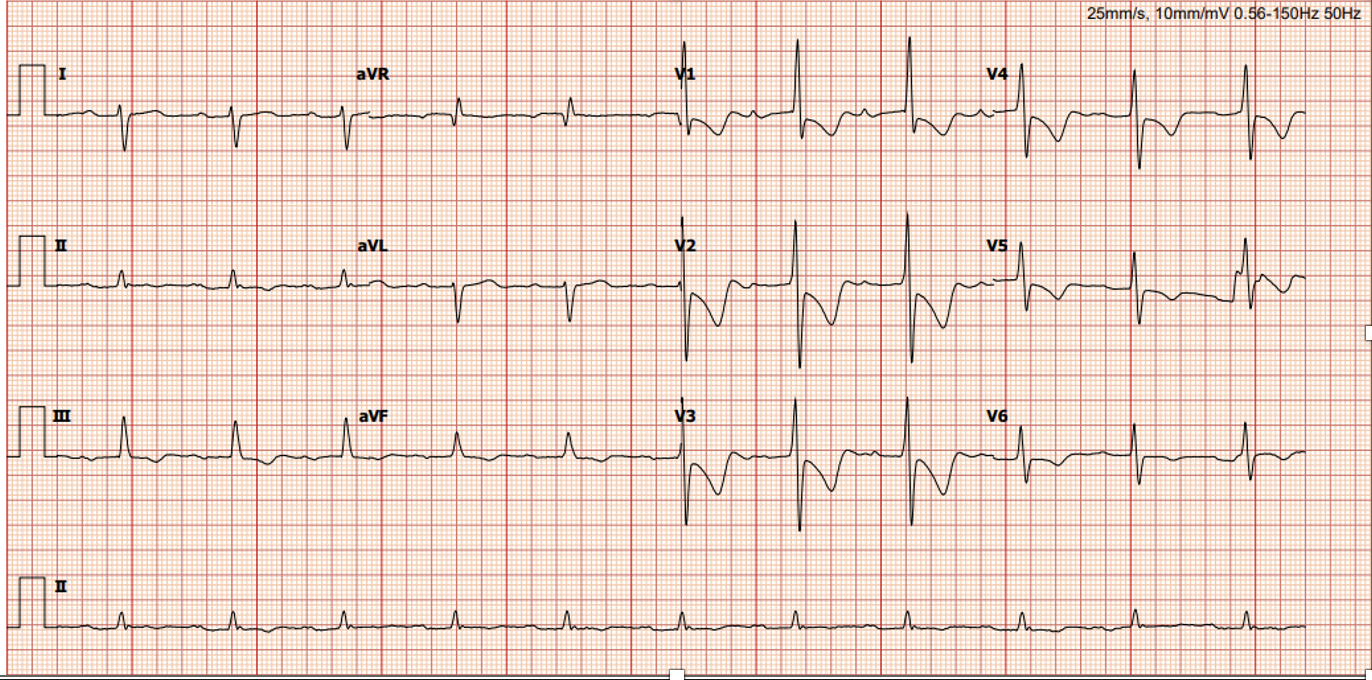
An EKG showed normal sinus rhythm, with tall R waves in V1 to V3 and T wave inversion in V1 to V6. A chest X-ray indicated cardiomegaly and an enlarged pulmonary artery, without congestion. An echocardiogram revealed normal biventricular systolic function, a dilated right atrium and right ventricle, moderate tricuspid regurgitation (TR), and a high probability of pulmonary hypertension.
 LM.mp4
LM.mp4
Relevant Catheterization Findings
A coronary angiogram revealed severe ostial left main (LM) stenosis, while the other parts of the coronary arteries were normal and plaque-free. External compression was suspected. Intravascular ultrasound (IVUS) confirmed severe stenosis with dynamic external compression, with the intima being free of plaque. Right heart catheterization showed pre-capillary pulmonary hypertension with a MPAP of 44 mmHg, a PCWP of 7 mmHg, and a PVR of 6.28 Wood units (WU).
Suwit-IVUS1.mp4
Suwit6.mp4
Interventional Management
Procedural Step
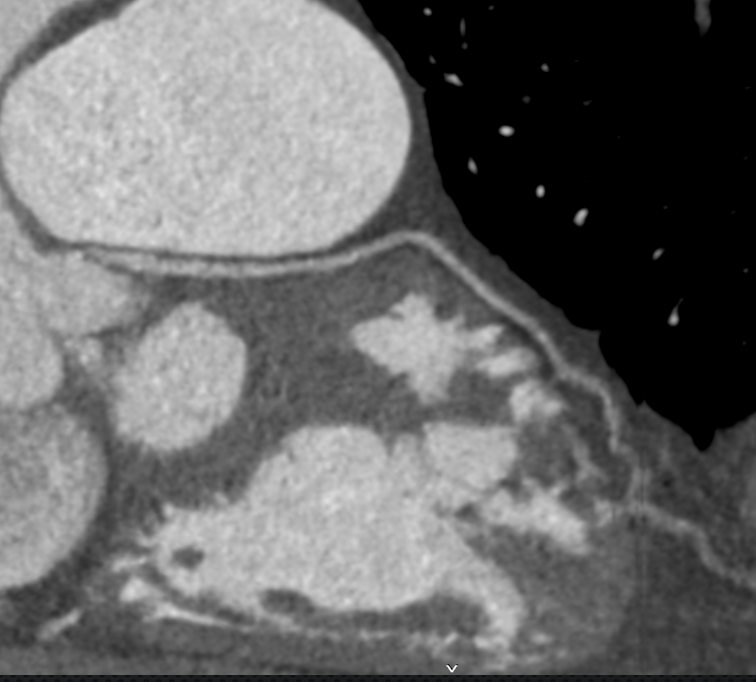
A CTA coronary artery scan showed compression of the left main coronary artery from an enlarged pulmonary artery. The heart team recommended undergoing PCI for the left main stenosis. A Guiding JL3.5 6F catheter was engaged to the left main, and a Sion Blue guidewire was passed to the distal LAD. IVUS was used to mark the left main ostium, and a floating wire was deployed to assist in the LM PCI. Direct stenting was performed using an Everolimus-eluting stent, sized 4.00 x 15 mm, at 12 atm. Post-dilatation was done with a non-compliant balloon, 5.0 mm, at 14 atm. The final angiogram showed good stent expansion, and IVUS confirmed good apposition with minimal stent protrusion.
PCI LM (12).mp4
PCI LM (8).mp4
Case Summary
His symptoms improved after the LM PCI. He was prescribed dual antiplatelet therapy for 6 months and a pulmonary vasodilator for the treatment of pre-capillary hypertension. This case demonstrated an unusual occurrence of left main stenosis due to an enlarged pulmonary artery, which was successfully treated with LM stenting.