CASE20240722_001
Tailoring a Lifeline with Double Kissing Mini Culotte
By Dena Karina Firmansyah, Arwin Saleh Mangkuanom, Doni Firman, Amir Aziz Alkatiri, Nanda Iryuza, Victor Giovannie Xaverison Rooroh, Muhammad Isra Tuasikal, Aris Munandar ZI
Presenter
Dena Karina Firmansyah
Authors
Dena Karina Firmansyah1, Arwin Saleh Mangkuanom1, Doni Firman1, Amir Aziz Alkatiri1, Nanda Iryuza1, Victor Giovannie Xaverison Rooroh1, Muhammad Isra Tuasikal1, Aris Munandar ZI1
Affiliation
National Cardiovascular Centre Harapan Kita, Indonesia1,
View Study Report
CASE20240722_001
Complex PCI - Bifurcation
Tailoring a Lifeline with Double Kissing Mini Culotte
Dena Karina Firmansyah1, Arwin Saleh Mangkuanom1, Doni Firman1, Amir Aziz Alkatiri1, Nanda Iryuza1, Victor Giovannie Xaverison Rooroh1, Muhammad Isra Tuasikal1, Aris Munandar ZI1
National Cardiovascular Centre Harapan Kita, Indonesia1,
Clinical Information
Relevant Clinical History and Physical Exam
A 33 year old male complained of worsening chest pain and fatigue with light activities such as walking 100 meter, giving a long speech in the last 3 months. He had 3 vessels and critical left main (LM) disease with in-stent restenosis (ISR) at proximal Left Anterior Descending (LAD) artery. On March 2024 at Regional Hospital, he underwent balloon angioplasty for ISR and had 1 stent implanted overlapped distal to the previous one. His Body Mass Index was 31.8 kg/m2 other findings were unremarkable.
 CAG 03:24.mov
CAG 03:24.mov
POBA ISR + PCI LAD 720.mov
Relevant Test Results Prior to Catheterization
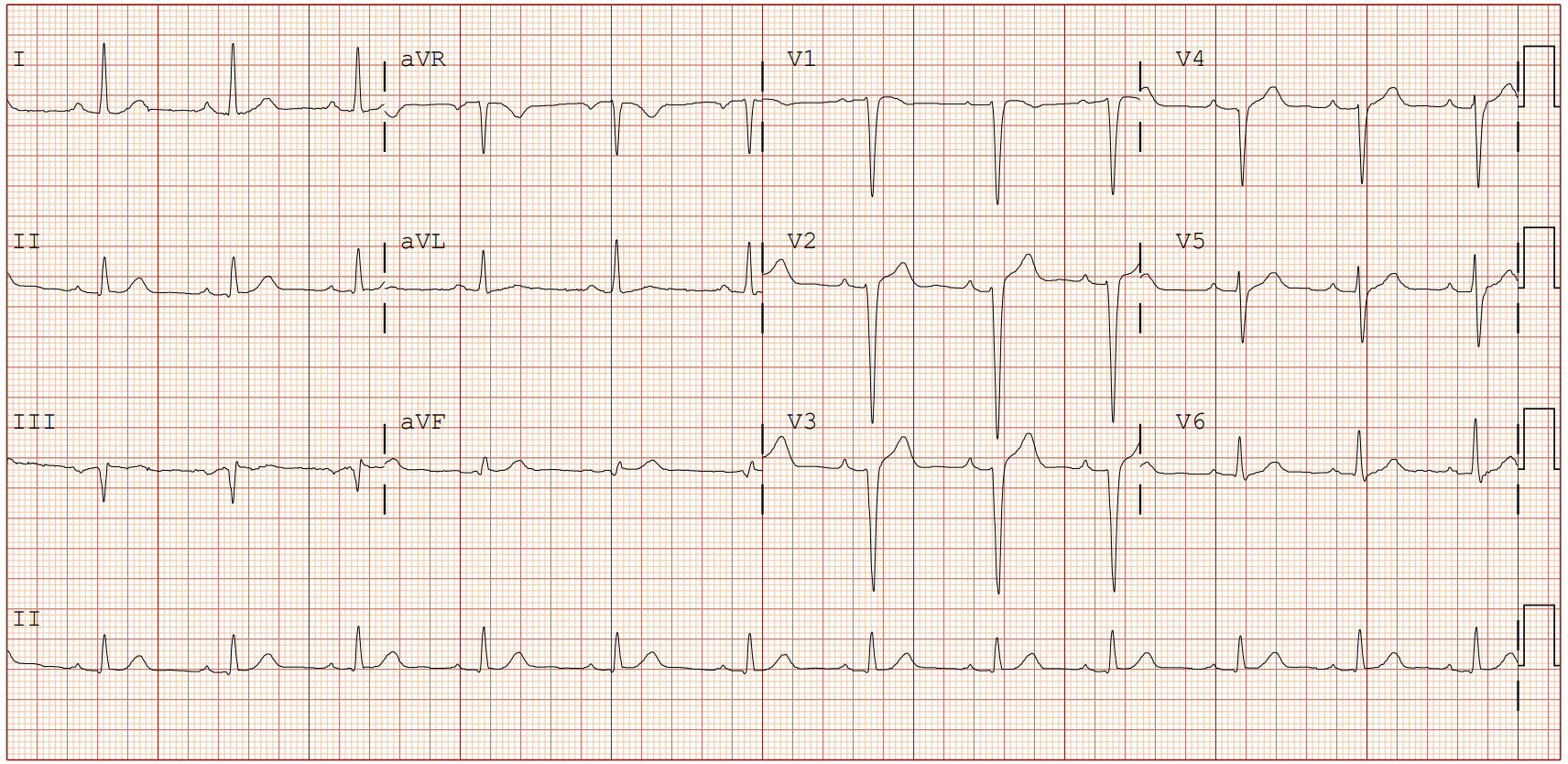
The Electrocardiogram showed Sinus Rhythm with poor R wave progression in V1-V5. Echocardiography revealed good ejection fraction (LVEF 57%), global normokinetic at rest and mild to moderate Aortic Regurgitation.
ECHO galih.mov
Relevant Catheterization Findings
Cannulation of Left Coronary Artery (LCA) was challenging due to pressure damping. With the side-hole EBU 3.5/6F (Medtronic) positioned just in front of the ostium, the angiography revealed progression of the lesion, i.e. subtotal occlusion of ostial-distal LM, subtotal occlusion of ostial LAD and Left Circumflex (LCX) artery with appearance of underflow to proximal-distal LAD and LCX (Medina 1,1,1).
CAG 0724.mov
Interventional Management
Procedural Step
Double wiring with workhorse wire to LCX served as anchor while the other wire crossed the lesion to LM-LAD.
wiring and prep 1.mov
IVUS LAD LCX Pre 1.mov
PCI LM LAD LCX 3.mov
Case Summary
Complex bifurcation lesion remains a challenge in PCI. Choosing the most appropriate strategy is crucial. The Double Kissing Mini-Culotte technique is reliable to treat the suitable complex bifurcation lesion. As a modification of classical culotte technique, it offers significant advantages including relatively easier and safer to perform, enhanced immediate procedural success in regards to morphological characteristics, and good clinical outcome.