CASE20240718_001
Mechanical Recanalization, Rotational Atherectomy and Stenting of the LAD
By Liudmila Ulyanova, Alexey Sozykin, Alexandr Shlykov, Emelianov Pavel, Natalya Novikova, Igor Lozovsky, Delikov Chingiz
Presenter
Emelianov Pavel
Authors
Liudmila Ulyanova1, Alexey Sozykin1, Alexandr Shlykov1, Emelianov Pavel1, Natalya Novikova1, Igor Lozovsky1, Delikov Chingiz1
Affiliation
Petrovsky National Research Center of Surgery; Petrovsky NRCS, Russian Federation1,
View Study Report
CASE20240718_001
Complex PCI - Calcified Lesion
Mechanical Recanalization, Rotational Atherectomy and Stenting of the LAD
Liudmila Ulyanova1, Alexey Sozykin1, Alexandr Shlykov1, Emelianov Pavel1, Natalya Novikova1, Igor Lozovsky1, Delikov Chingiz1
Petrovsky National Research Center of Surgery; Petrovsky NRCS, Russian Federation1,
Clinical Information
Relevant Clinical History and Physical Exam
A patient with angina at the level of functional class 3 was admitted to our clinic for coronary angiography and to decide on further treatment tactics. Coronary angiography revealed RCA and LAD occlusions. At the first stage, the patient underwent mechanical recanalization and implantation of 3 DES in the RCA It is recommended to perform recanalization and stenting of the LAD in a planned manner.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
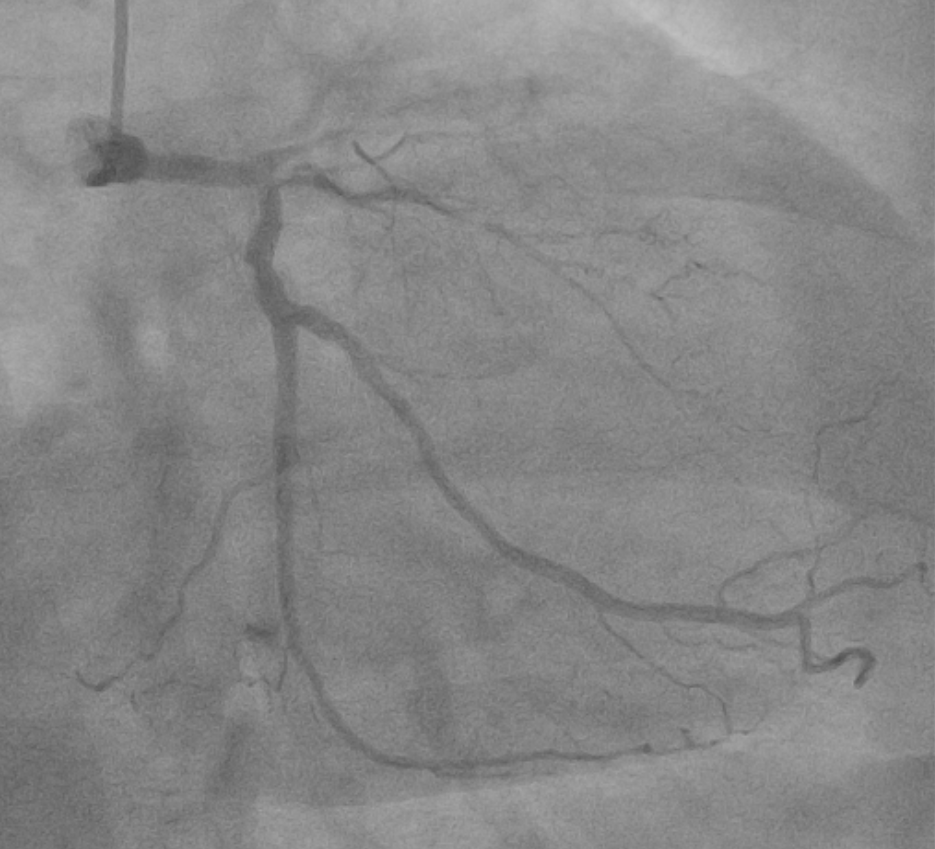
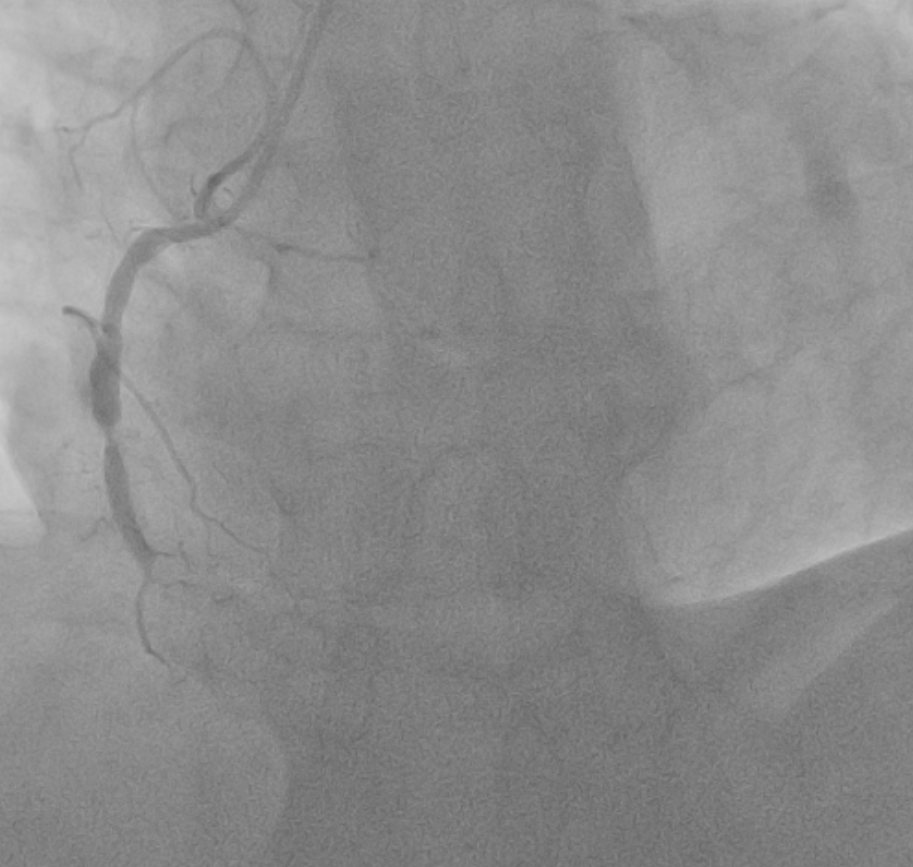
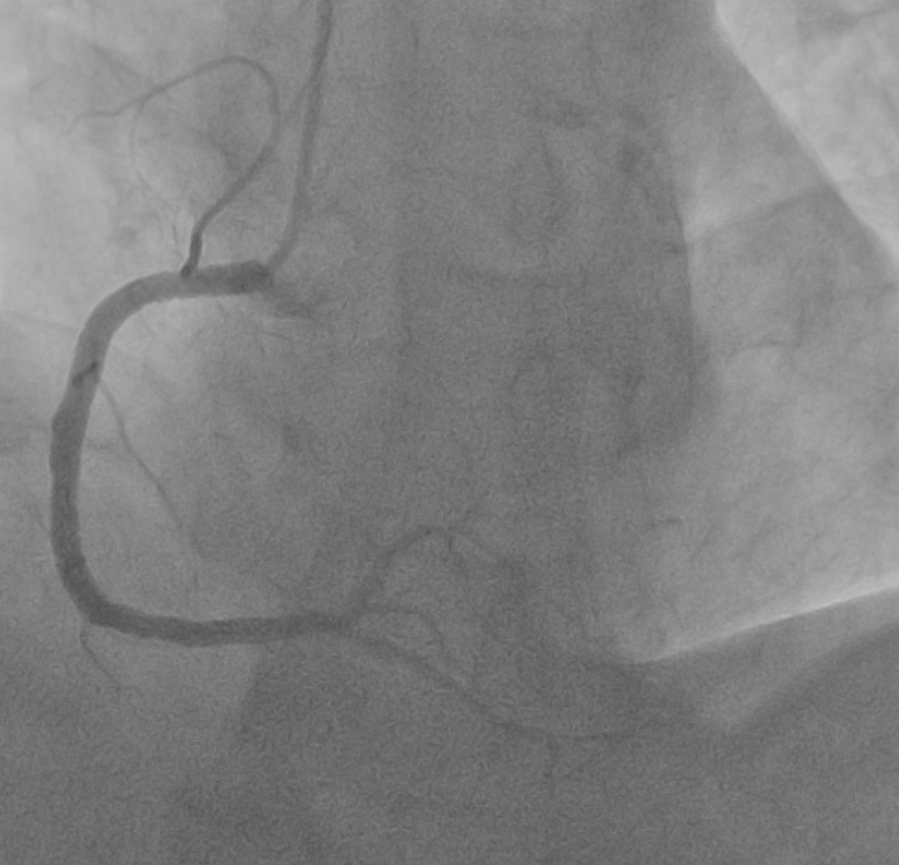
Typeof coronary blood supply: right. LM have irregular contours. LAD: with irregular contours, occluded in themiddle segment. LCx: with uneven contours throughout. RCA: with unevencontours, a stented area is visualized in the proximal and middle segments,without signs of restenosis and thrombosis

Interventional Management
Procedural Step
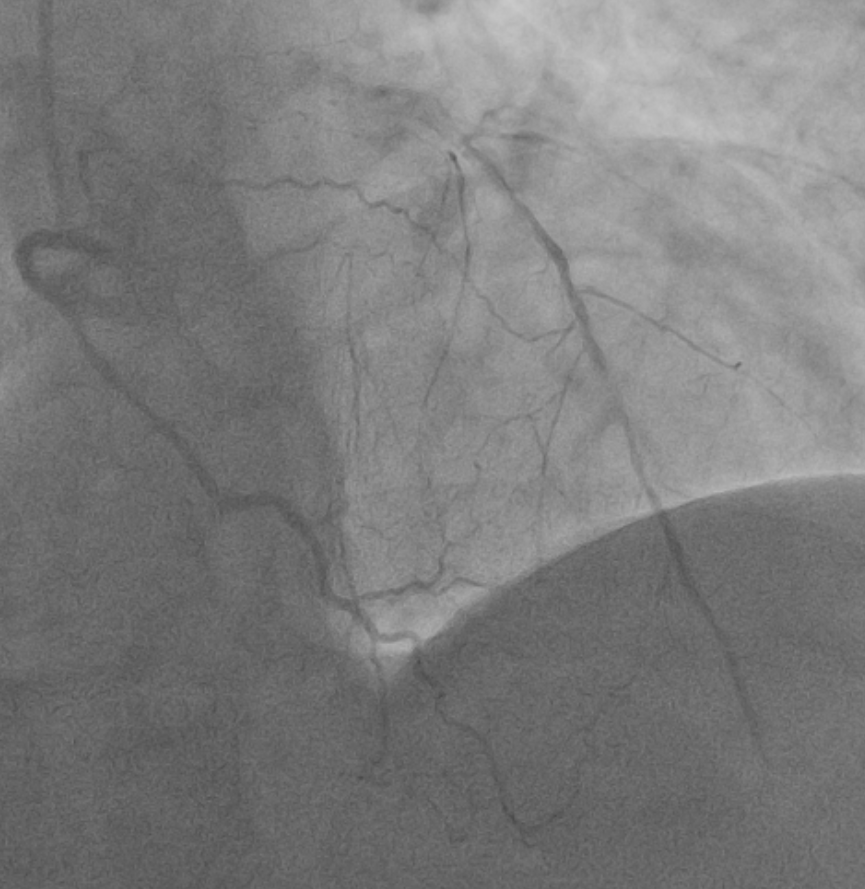
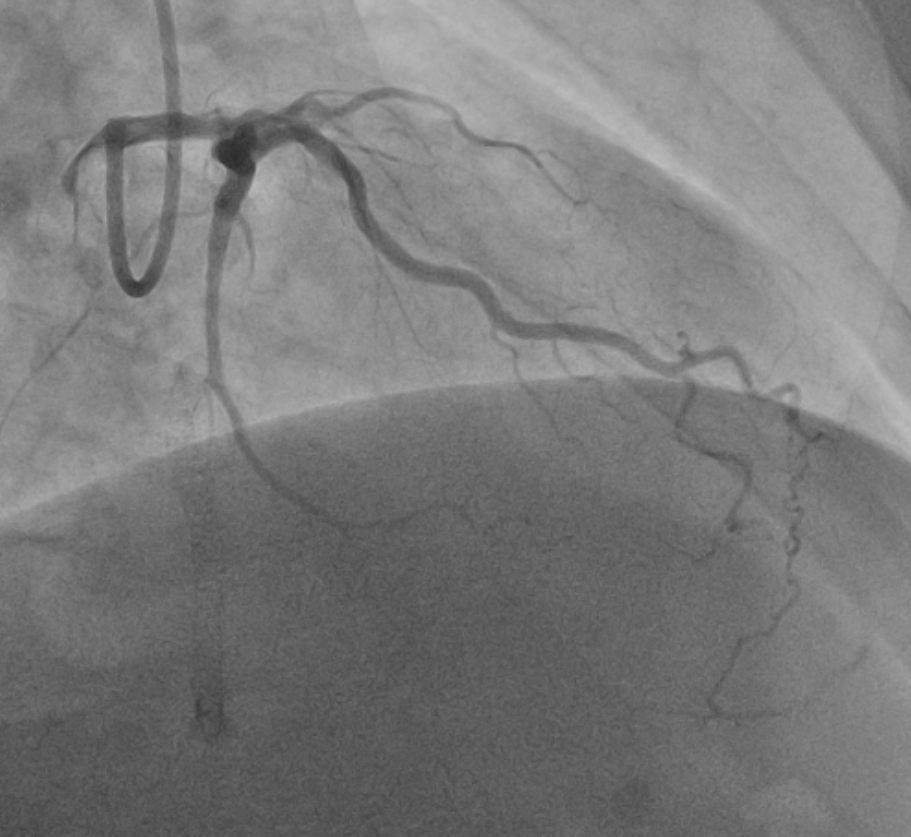
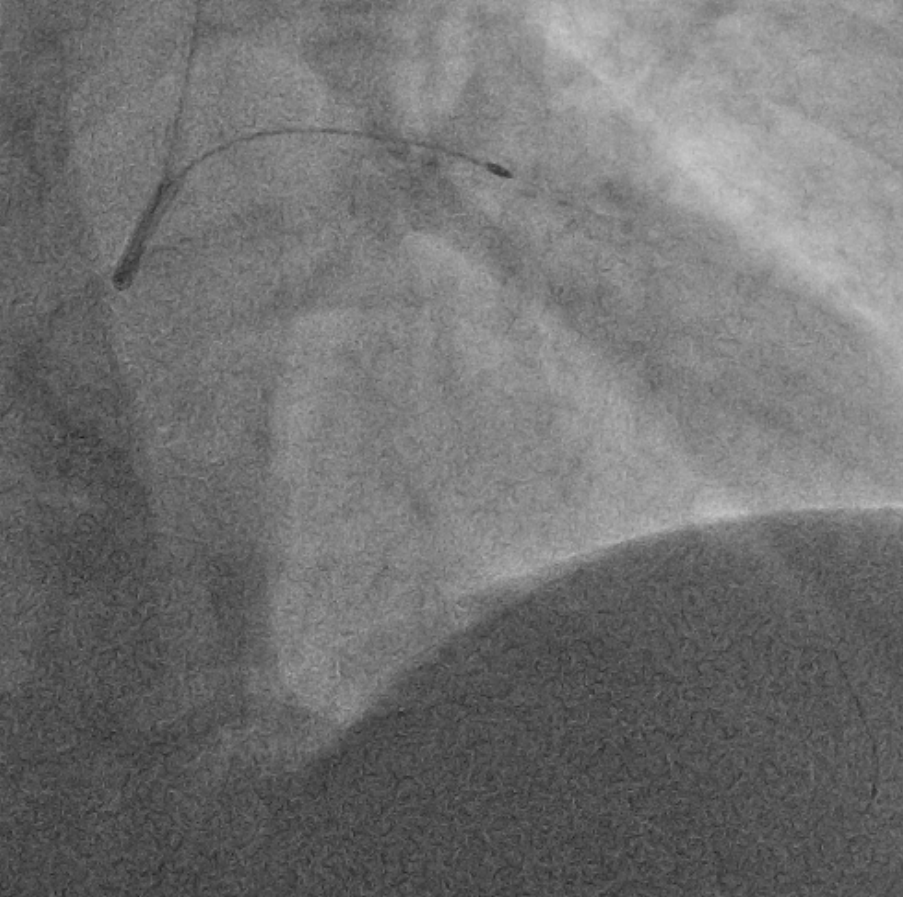
Performed mechanical recanalization of the LAD. The coronary guidewire was placed in the distal segment. However, balloon catheters of various diameters could not be brought into the site of occlusion. The coronary guidewire was changed to RotaWire, and rotational atherectomy was successfully performed with 1.25mm and 1.5mm burs. Balloon catheters 2.5x20mm, 2.75x15mm were used for predilation at the site of stenosis in the middle segment of the LAD. Successive implantation of DES 3.0*38 mm and 3.0*34 mm was performed in the middle and proximal segments of the LAD. OCT was performed, according to which incomplete expansion of the implanted stent in the middle segment was detected. Postdilatation was performed with balloon catheters NC 3.5x15mm, pressure up to 20 atm. Control angiography shows extravasation of the contrast agent. Attempts to perform hemostasis using a balloon catheter were unsuccessful. Sequential implantation of Papirus 4.0*20mm and Papirus 3.5*20mm stent grafts was performed in the proximal and middle segments of the LAD. With control fluoroscopy, the divergence of the sheets of the pericardium is visualized. Due to unstable hemodynamics and divergence of the pericardial layers, a decision was made to puncture and drain the pericardial cavity. 8F drain installed. Received 400 ml of hemorrhagic fluid. Control angiography showed no extravasation of the contrast agent, blood flow through the TIMI III artery. Stable hemodynamics.


Case Summary
Knowledge of the treatment methods of the procedures helps the operator to choose the most appropriate treatment method and achieve a successful stenting result. Well-coordinated work of the entire team is a prerequisite for successful combating PCI situations. Availability and rapid access to emergency tools are often critical.