CASE20240713_005
An Unsacrificeable Sidebranch
By Choutchung Tinakorn Na Ayudhya
Presenter
Choutchung Tinakorn Na Ayudhya
Authors
Choutchung Tinakorn Na Ayudhya1
Affiliation
King Chulalongkorn Memorial Hospital, Thailand1,
View Study Report
CASE20240713_005
Complex PCI - Bifurcation
An Unsacrificeable Sidebranch
Choutchung Tinakorn Na Ayudhya1
King Chulalongkorn Memorial Hospital, Thailand1,
Clinical Information
Relevant Clinical History and Physical Exam
A 60 year-old man
Known case HT and dyslipidemia on medications presented with intermittent progressive chest pain on exertion for 3 months. He had no orthopnea, no PND, No syncope.
He was diagnosed with CCS and CAG showed triple vessel disease without LM disease. He underwent PCI to RCA and was scheduled for stage PCI to LAD lesion.
Physical examination BP 125/86 mmHg HR 71/min RS no crepitation CVS normal s1s2 no murmur.
Relevant Test Results Prior to Catheterization
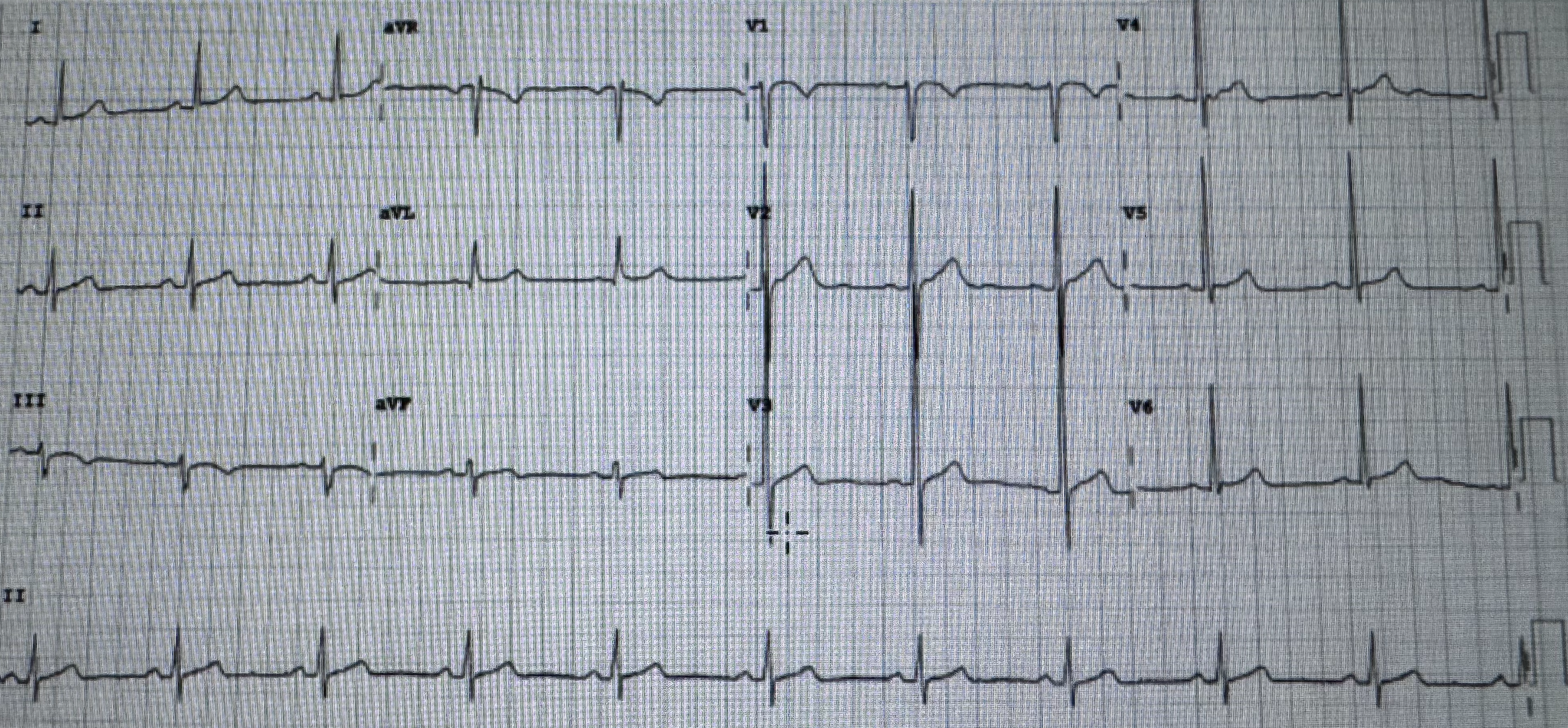
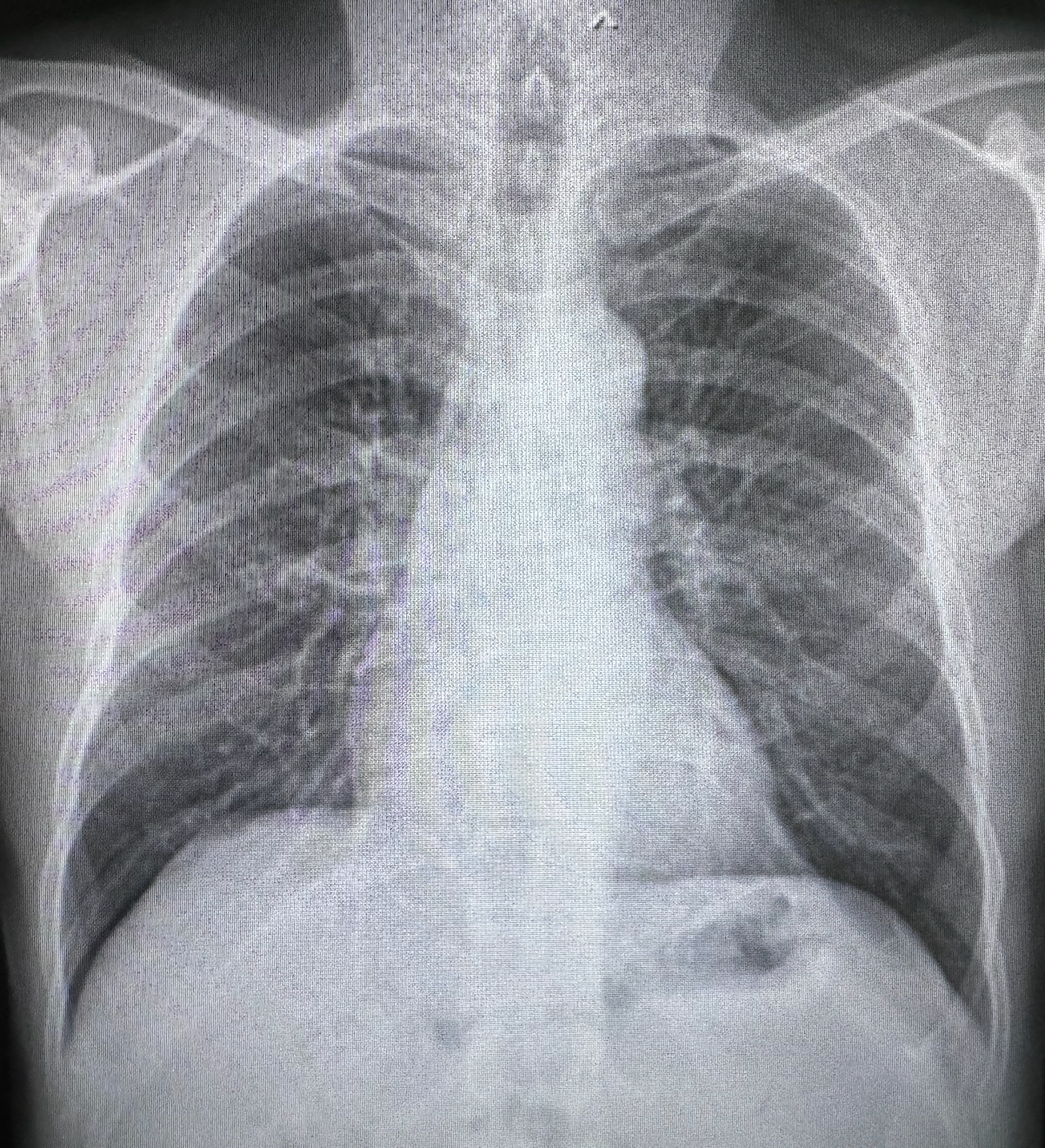
EKG: showed sinus rhythm rate 62/min normal axis no chamber enlargement no definite ST-T changeCXR: normal heart size without congestionEcho: Normal LV size and LV wall thickness. Normal LV systolic function. LVEF = 76% by Teichholz without RWMAs. No significant valvular abnormalities.
 A4C.MOV
A4C.MOV
PLAX.MOV
PSAX.MOV
Relevant Catheterization Findings
CAG via right femoral approach using 6Fr system showed patent stents from mid to distal RCA without ISR. There was 80% stenosis at mid LAD and 90% stenosis at ostial DG2. (Bifurcation lesion medina 1-1-1) and there was 70% stenosis at proximal Lcx.
1.mp4
3.mp4
6.mp4
Interventional Management
Procedural Step
A 6 Fr. XB3 guiding catheter was engaged into LCA. A Sion blue wire could advance into distal LAD. However runthrough wire could not advanced into DG2. A Fielder FC wire with Crusade type R microcatheter was used to advanced wire into DG2. Crusade was removed using Kusabi trapping balloon. Pre-dilated was done at mid LAD and postal DG2 with SC balloon 2.0 x 15mm the IVUS from LAD and DG was done which showed subintimal wiring in the proximal part of DG2. Pre-dilated at mid LAD was done with NC balloon 2.75x15 mm at 18-20 ATM. We planned to do upfront 2 stent at LAD-DG2 bifurcation using mini crush technique due to dissection and subintimal wiring at proximal DG2. A DES 2.25x26 mm was deployed at proximal DG2 with 2 mm profusion into LAD and then was crushed using NC 2.75 balloon. A DES 2.75x26 mm was deployed at mid LAD. DG2 was rewire with runthrough wire and crusade microcatheter then jailed wire and crusade microcatheter was removed. KBI was done with NC balloon 2.5x15 in DG2 and 3.0x15 mm in LAD. POTs was done with NC balloon 3.5x8 mm at mid LAD. IVUS was done post PCI which showed acceptable stent expansion in both LAD and DG without evidence of complications.
13.mp4
29.mp4
34.mp4
Case Summary
A case with bifurcation lesion with very stenosis at ostial lesion of the small side branch, wiring into side branch may be very difficult and challenging. Using dual lumen microcatheter could increase support and increase chance of successfully wiring into the side branch. Sometimes subintimal wiring could be done when wiring in the true lumen seems to be impossible task with a successful PCI results.