CASE20240711_002
A Case of Guiding Catheter Induced Spiral Dissection: Use of Real-Time IVUS Guided Wiring and Cutting Balloon Fenestration
By Guo Shu Huang
Presenter
Guo Shu Huang
Authors
Guo Shu Huang1
Affiliation
Asia University Hospital, Taiwan1,
View Study Report
CASE20240711_002
Complication Management - Complication Management
A Case of Guiding Catheter Induced Spiral Dissection: Use of Real-Time IVUS Guided Wiring and Cutting Balloon Fenestration
Guo Shu Huang1
Asia University Hospital, Taiwan1,
Clinical Information
Relevant Clinical History and Physical Exam
A 60+ years-old female presented with NSTEMI
Chest tightness and dyspnea on exertion in recent days
Medication history of hypertension Stable hemodynamic status at presentationCATH was arranged on the next morning
Medication history of hypertension Stable hemodynamic status at presentationCATH was arranged on the next morning
Relevant Test Results Prior to Catheterization
Elevated Troponini-I level
Relevant Catheterization Findings
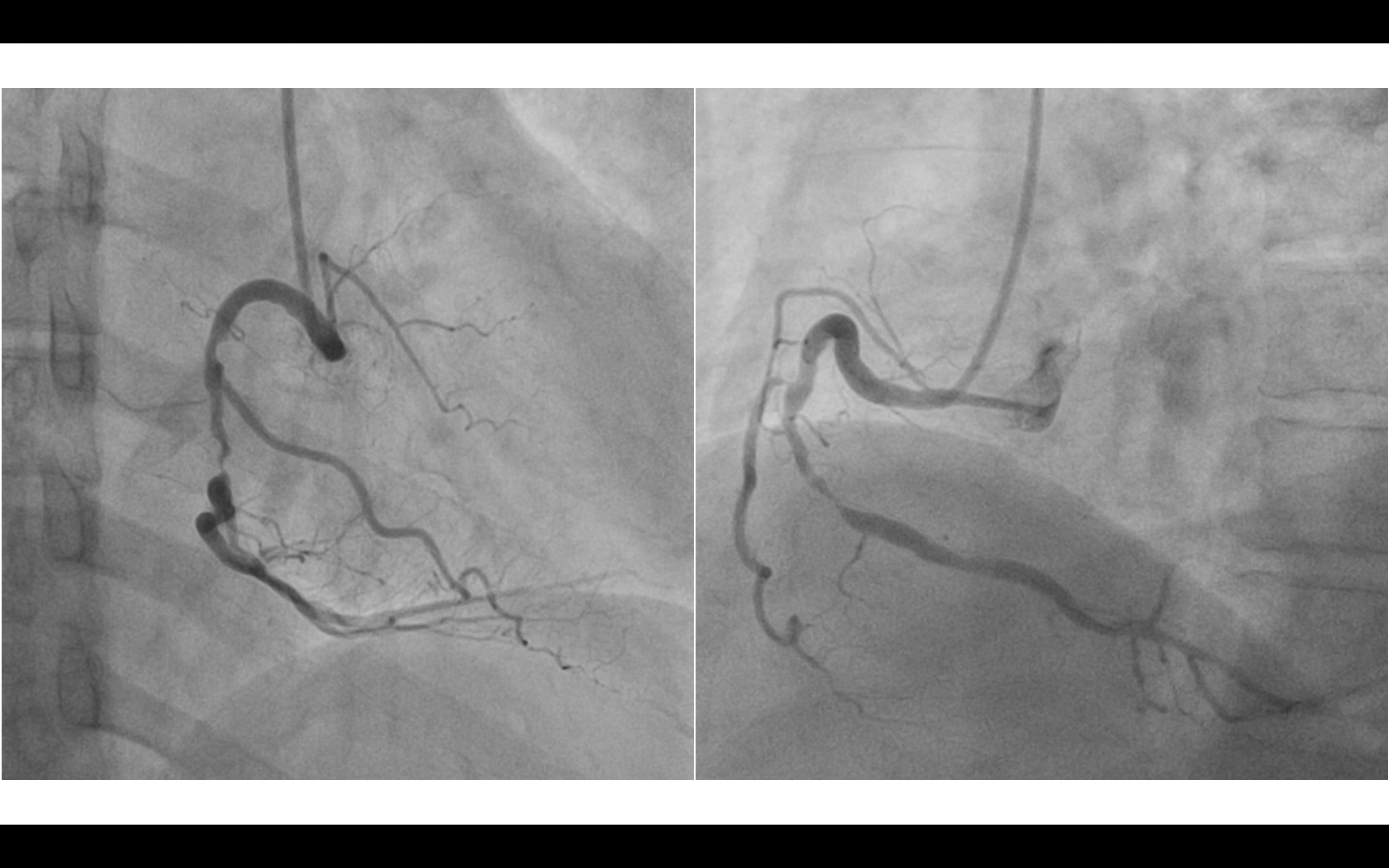
RCA: critical stenosis at middle portion
Interventional Management
Procedural Step
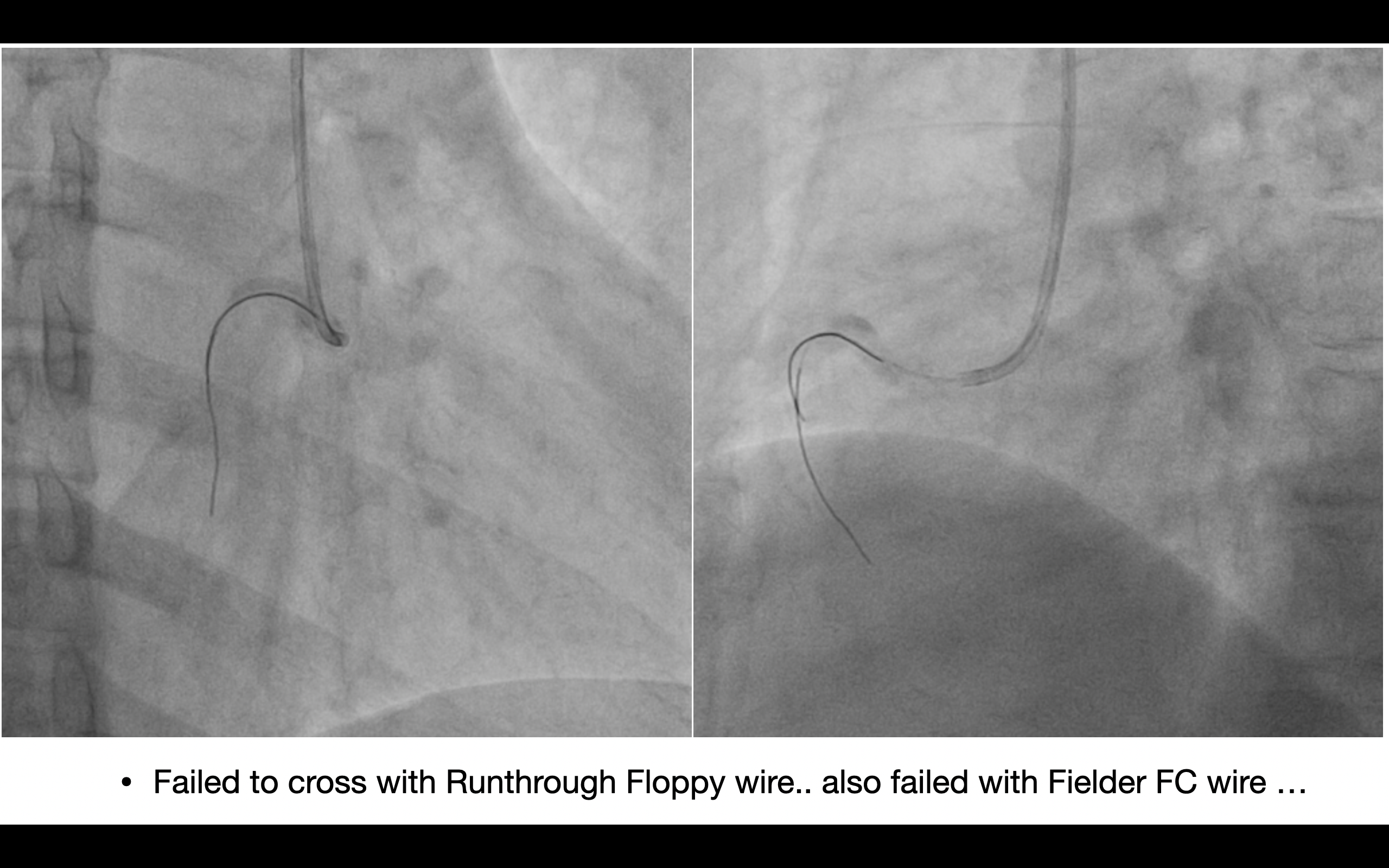
Initial single wiring with Runthrough floopy wire was failed to cross the critical lesion. Buddy wiring with Fielder FC wire also cannot cross through the critical stenosis lesion. Wire motion indicated false lumen wiring. Angiography showed spiral dissection with unknown origin of the dissection. Tried Buddy wire wiring again, but failed to cross into true lumen.
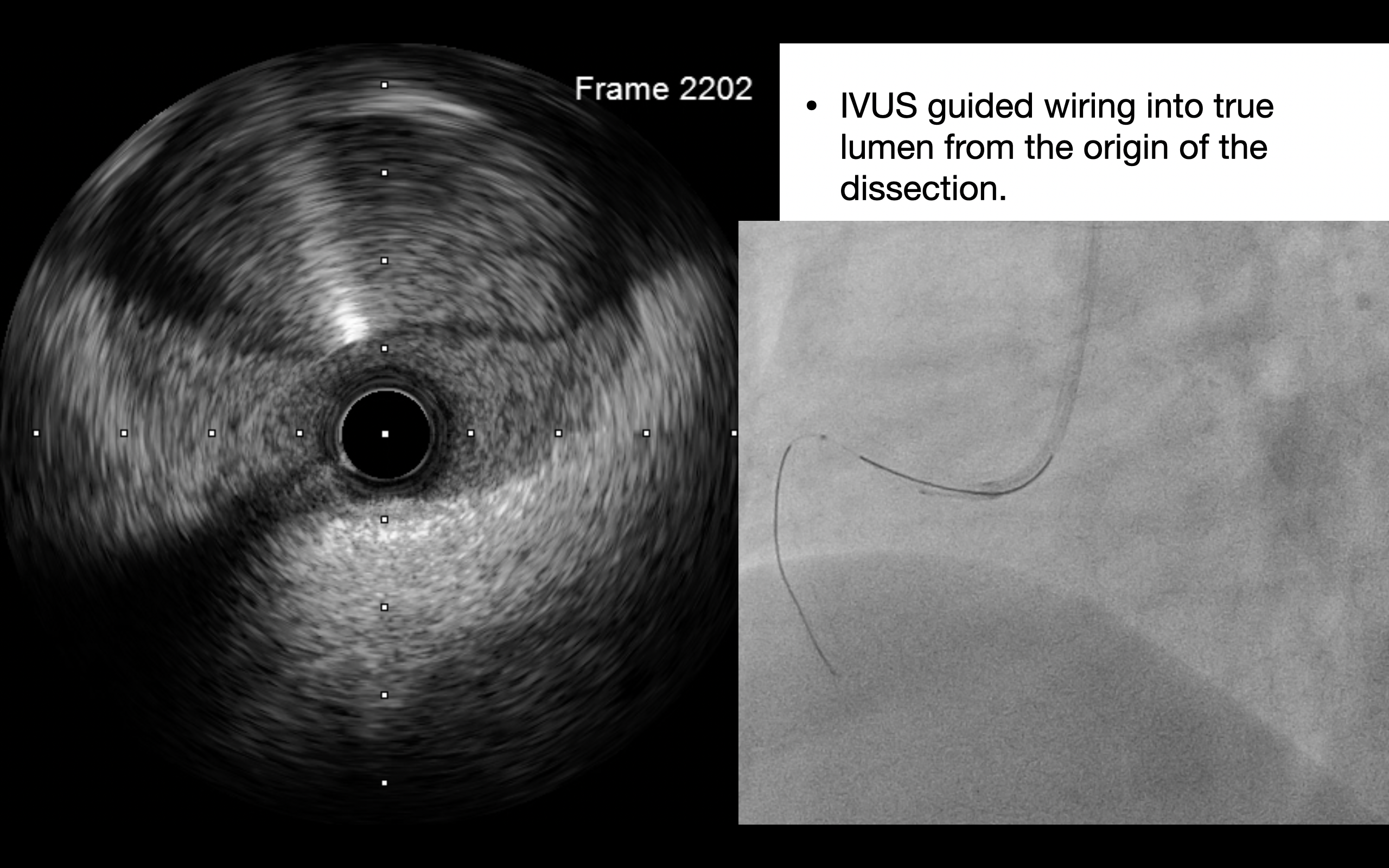
Under real time IVUS guided wiring, origin of the dissection was discovered and the wire was successfully cross into the true lumen.
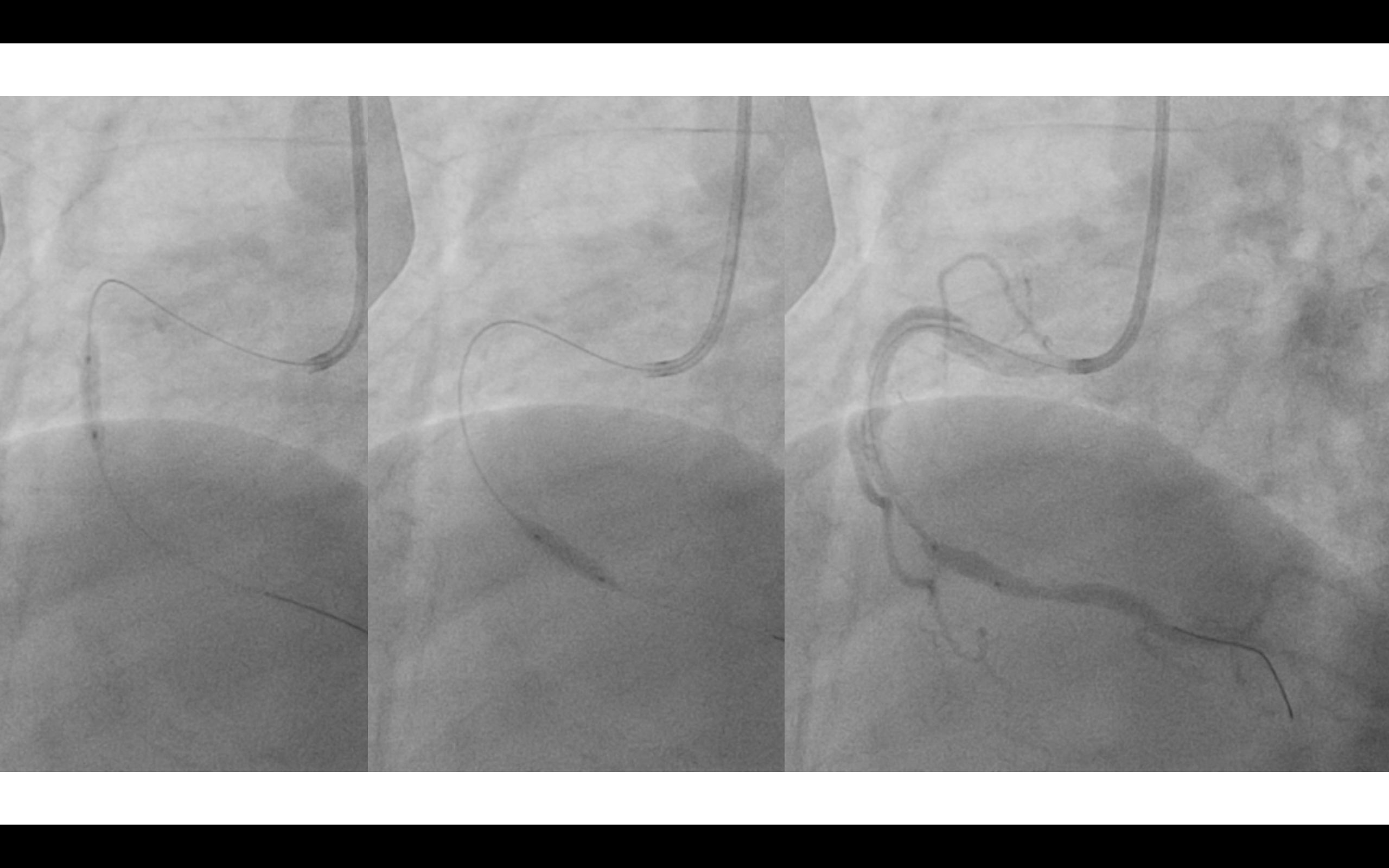
Due to IVUS showed huge hematoma, cutting balloon fenestration to limit the hematoma expansion and extension.
Finally, successful stenting the critical lesion and the spiral dissection.
Case Summary
Real time IVUS guided wiring can be done with 6Fr guiding catheter. Beneficial of IVUS guided wiring included unveil dissection origin, confirmation of the wire position, and shortened procedure time.Cutting balloon fenestration can limited the hematoma extension and/or expansion ante-gradely and/or retrogradely.